
Vitamin D Deficiency Symptoms: A 2026 Evidence-Based Guide
Vitamin D Deficiency Symptoms: A 2026 Evidence-Based Guide
By the HealthPerk Editorial Team · Last updated: May 2026
Quick Answer
What are the main vitamin D deficiency symptoms?
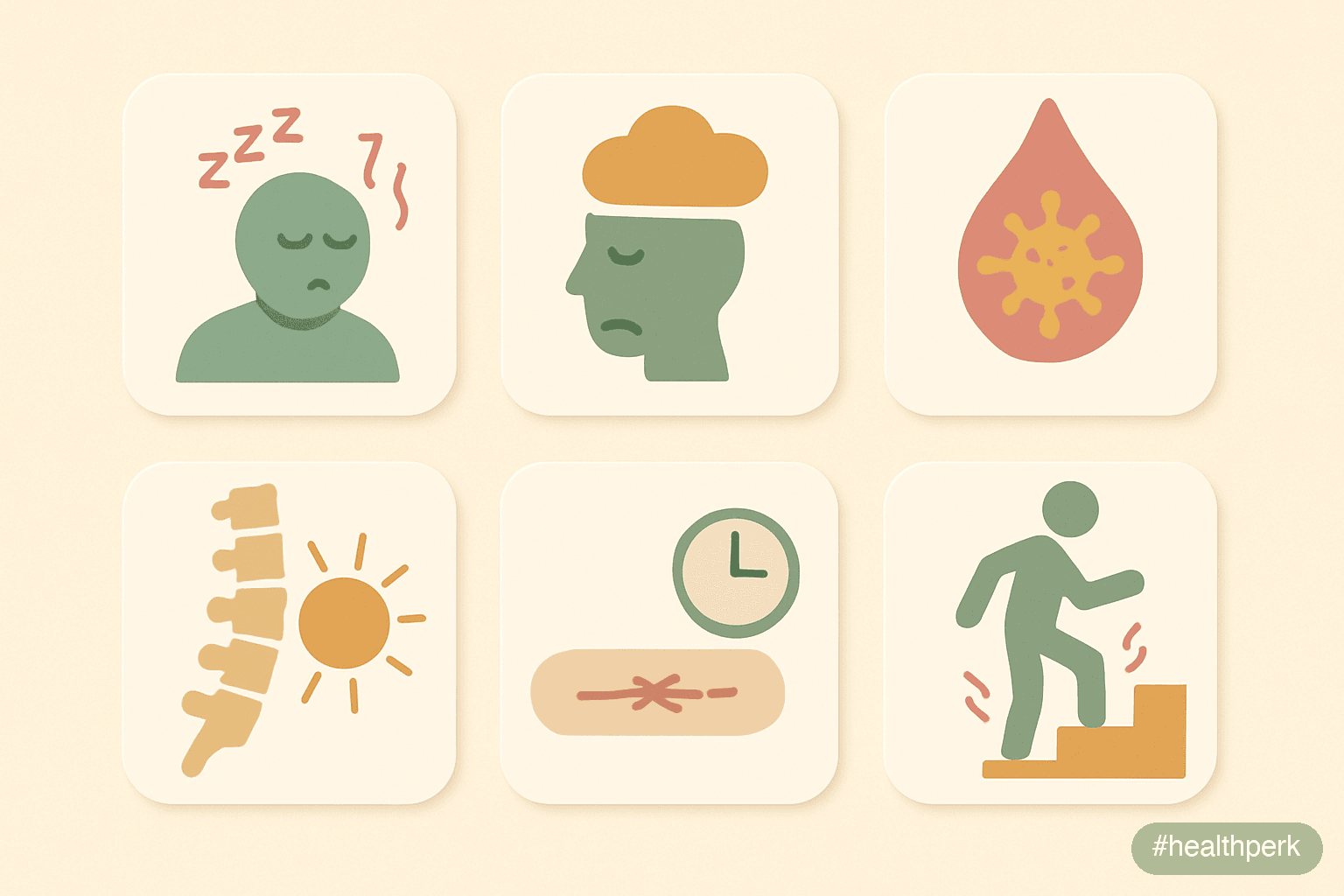
Vitamin D deficiency is usually quiet. The most reproducible clinical signs in adults are persistent fatigue out of proportion to sleep, diffuse musculoskeletal aches (especially around the lower back, hips, and shins), proximal muscle weakness that makes stairs feel harder, low mood and lower stress tolerance through winter, more-frequent upper-respiratory infections than peers, slow wound healing, and — at lower thresholds — bone pain or stress fractures. The decisive test is a serum 25-hydroxyvitamin D (25(OH)D) level: under 12 ng/mL (30 nmol/L) is frank deficiency, 12–20 ng/mL is insufficiency, 20–30 ng/mL is borderline-adequate, and 30+ ng/mL is replete by most guidelines in 2026. Symptoms cluster rather than appear singly, and they overlap heavily with sleep debt, stress, and hypothyroidism — which is why diagnosis is a blood test, not a checklist.
A short orientation table:
| Question | Short answer |
|---|---|
| Definitive test | Serum 25-hydroxyvitamin D (25(OH)D) |
| Deficient | <12 ng/mL (<30 nmol/L) |
| Insufficient | 12–20 ng/mL (30–50 nmol/L) |
| Adequate (IOM) | 20–50 ng/mL (50–125 nmol/L) |
| Endocrine Society "sufficient" | 30–50 ng/mL (75–125 nmol/L) |
| RDA, adults 19–70 | 600 IU/day (15 mcg) |
| RDA, adults 71+ | 800 IU/day (20 mcg) |
| Tolerable Upper Intake Level | 4,000 IU/day (100 mcg) without medical oversight |
| Form to prefer | Cholecalciferol (D3) over ergocalciferol (D2) |
| Take with | A fat-containing meal (fat-soluble vitamin) |
The phrase vitamin d deficiency symptoms consistently sits in the top-five supplement queries in 2026, and the search interest tracks a real epidemiological fact: a sizeable minority of adults in most temperate countries spend at least part of the year below the 20 ng/mL adequacy threshold. The 2017–2018 NHANES cycle in the United States, the most recent fully analyzed pre-pandemic data still cited by the NIH Office of Dietary Supplements in 2026, estimated that roughly 18% of US adults were below 20 ng/mL and about 5% were below 12 ng/mL, with substantially higher rates in Black and Hispanic adults, older adults, and adults with obesity.
What the search interest tends to miss is how indirect the symptom picture is. Vitamin D operates through a nuclear receptor expressed in nearly every tissue in the body and acts upstream of calcium homeostasis, immune regulation, and muscle function. Its deficiency consequences are therefore distributed and subtle, not focal and obvious. This guide walks through what vitamin D actually is, the cluster of symptoms that should prompt testing, the dosing numbers that are defensible in 2026, what the evidence does and does not support for immunity, and a practical framework for deciding whether you personally need a supplement.
Table of Contents
- Vitamin D: What It Actually Is and Why Status Matters More Than Intake
- Low Vitamin D Symptoms in Adults: The Quiet Cluster Most People Miss
- How Much Vitamin D Per Day: The RDA, the Endocrine Society Number, and What Trials Used
- Vitamin D Benefits for Immunity: What 2026 Evidence Actually Supports
- Do I Need Vitamin D Supplements? A Decision Framework Based on Sun, Skin, and Latitude
- Frequently Asked Questions
- References
Vitamin D: What It Actually Is and Why Status Matters More Than Intake
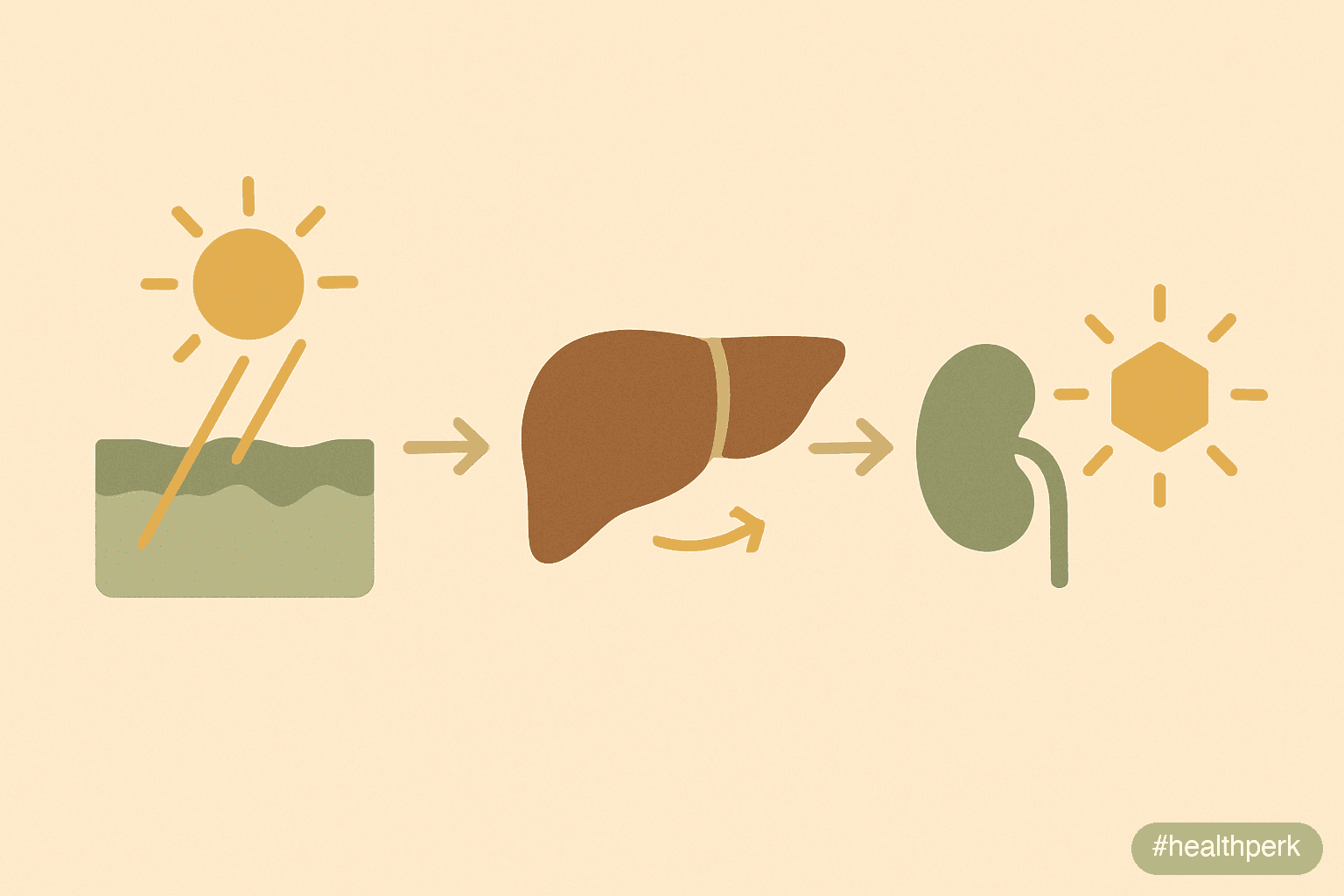
Vitamin D is, strictly speaking, not a vitamin at all in the classical sense. A vitamin is a compound the body cannot make and must obtain from diet. Vitamin D can be synthesized in the skin from 7-dehydrocholesterol when UVB radiation between roughly 290 and 315 nanometers strikes the cells of the epidermis. It is more accurately described as a secosteroid hormone with two relevant forms: ergocalciferol (D2, from fungal and plant sources) and cholecalciferol (D3, from animal sources and from human skin). Both are biologically inactive until processed.
The activation pathway is two-step. The liver hydroxylates D3 (or D2) into 25-hydroxyvitamin D, abbreviated 25(OH)D and also called calcidiol. This is the circulating storage form and is what lab tests measure. The kidney then performs a second hydroxylation on demand, producing 1,25-dihydroxyvitamin D — calcitriol — which is the hormonally active form that binds the vitamin D receptor (VDR) in target tissues.
Two practical implications follow from this biology:
- Intake and status are not the same number. Two adults taking identical 1,000 IU daily can land at very different 25(OH)D levels. Differences in body composition (vitamin D is fat-soluble and sequesters in adipose tissue), skin pigmentation (higher melanin reduces cutaneous synthesis), sun exposure, age (cutaneous synthesis declines with age), genetic variation in vitamin-D-binding protein, and gut absorption efficiency all contribute. Status — the 25(OH)D level — is what matters clinically. Intake is the lever you control.
- The active hormone is tightly regulated by the kidney. Most adults cannot self-induce frank toxicity from sun alone; the skin down-regulates synthesis as exposure continues. Toxicity from oral supplementation is possible but generally requires sustained intake well above 10,000 IU/day for months, or single very large doses. The Tolerable Upper Intake Level in the US is 4,000 IU/day for adults; this is a conservative ceiling chosen with a wide safety margin.
The functions of the activated hormone are extensive. The textbook role is calcium absorption from the gut and bone mineralization through partnership with parathyroid hormone. The expanded role, recognized increasingly since the early 2000s, includes immune modulation (both innate and adaptive), muscle fiber function, glucose metabolism, and gene expression across hundreds of target genes. These distributed functions are why low status produces a distributed, low-grade symptom cluster rather than a single dramatic deficiency syndrome.
Low Vitamin D Symptoms in Adults: The Quiet Cluster Most People Miss
Low vitamin D symptoms in adults are the textbook example of a deficiency that hides in plain sight. The symptoms are real but they overlap completely with the symptoms of sleep debt, chronic stress, hypothyroidism, depression, iron deficiency, and ordinary winter dimness. This overlap is why a defensible diagnosis is always confirmed by a 25(OH)D blood test rather than inferred from a checklist alone.
The most commonly reported features in adults with insufficiency (12–20 ng/mL) or deficiency (<12 ng/mL):
- Persistent fatigue that does not resolve with extra sleep and is not explained by anemia, thyroid disease, or sleep apnea.
- Diffuse musculoskeletal aches, most often in the lower back, hips, pelvic girdle, knees, and shins. Pain is typically bilateral, dull, and worse on rising in the morning.
- Proximal muscle weakness, classically noticed as needing the handrail on stairs, harder time rising from a chair without using arms, or trouble lifting groceries to a high shelf. This pattern is more specific to vitamin D than the other features.
- Bone tenderness when firm pressure is applied to the sternum, anterior tibia, or pelvis. Severe and prolonged deficiency leads to osteomalacia (adult equivalent of rickets), which can produce frank bone pain and increase risk of low-impact fractures.
- Low mood, lower stress tolerance, and a winter-aggravated dip in motivation that is not reliably distinguishable from seasonal affective disorder by symptoms alone. The association of low 25(OH)D with depressive symptoms is consistent across cross-sectional studies, though randomized supplementation trials show smaller effects on mood than the observational data suggested.
- More-frequent upper-respiratory tract infections than peers — colds that come more often, last longer, or are subjectively heavier. This signal is modest at the population level but reproducible.
- Slower wound healing and a sense that minor cuts or surgical sites take longer to close than expected.
- Hair shedding is a frequently asserted symptom in popular content; the evidence base is thinner than for the musculoskeletal cluster, and other causes (iron, thyroid, telogen effluvium after stress) are usually more relevant.
- Worsening glycemic control in adults with prediabetes or type 2 diabetes — an association rather than a direct symptom, but worth flagging for adults with risk factors.
Risk factors that quietly drive low status:
- Living at latitudes above about 35° (north or south) from October through March, when UVB is too oblique to drive meaningful skin synthesis regardless of how much "sun" reaches the ground.
- Darker skin pigmentation: higher melanin attenuates UVB penetration. Black adults in the US carry roughly 4–5 times higher rates of deficiency than non-Hispanic White adults in NHANES data.
- Spending most daylight hours indoors (office work, remote work, shift work).
- Routine sunscreen use above SPF 15 across all exposed skin (effective sun protection is also effective vitamin D synthesis suppression).
- Body mass index (BMI) over 30: vitamin D distributes into adipose tissue and circulating 25(OH)D drops at any given intake.
- Older age, particularly above 65, due to thinner skin and lower 7-dehydrocholesterol availability.
- Malabsorption: celiac disease, Crohn's disease, gastric bypass, cystic fibrosis, or chronic pancreatitis.
- Vegan diets without fortified foods or supplements (vitamin D3 has historically required animal sources, though lichen-derived D3 is widely available in 2026).
- Anticonvulsants, long-term oral corticosteroids, and certain antiretrovirals accelerate vitamin D catabolism.
How to investigate: a single 25-hydroxyvitamin D blood test, ideally drawn at the end of winter (February–April in the Northern Hemisphere) when status is at its annual nadir. Reflex testing of calcium, phosphate, and parathyroid hormone is sometimes ordered if the 25(OH)D is markedly low; vitamin D toxicity testing (1,25(OH)2D and total/ionized calcium) is reserved for adults with confirmed hypercalcemia or excessive supplementation history.
How Much Vitamin D Per Day: The RDA, the Endocrine Society Number, and What Trials Used

How much vitamin D per day is one of the most contested numbers in nutrition because the same evidence base supports two different framings. The Institute of Medicine (IOM, now the National Academies) sets numbers calibrated to bone health in the general population. The Endocrine Society sets numbers calibrated to achieving 25(OH)D levels of 30 ng/mL or higher in clinical patients. Both are defensible; they answer different questions.
The IOM Recommended Dietary Allowances (still the basis of US nutrition labeling in 2026):
- Infants 0–12 months: Adequate Intake of 400 IU/day (10 mcg).
- Children and adults 1–70 years: RDA 600 IU/day (15 mcg).
- Adults 71+ years: RDA 800 IU/day (20 mcg).
- Pregnancy and lactation: 600 IU/day.
- Tolerable Upper Intake Level (UL): 1,000 IU/day (infants 0–6 months), 1,500 IU/day (6–12 months), 2,500–3,000 IU/day (1–8 years), 4,000 IU/day (9+ years).
The Endocrine Society 2024 guideline update, written for clinicians treating patients at risk of deficiency:
- Adults at risk (older adults, dark skin, limited sun exposure, obesity, malabsorption): empirical supplementation of 1,500–2,000 IU/day to maintain 25(OH)D above 30 ng/mL.
- Obese adults (BMI ≥30): typically require 2–3 times the standard dose to reach the same serum level.
- Treatment of confirmed deficiency (<20 ng/mL): a loading approach of 6,000 IU/day for 8 weeks (or weekly 50,000 IU for 8 weeks) followed by maintenance of 1,500–2,000 IU/day, with retest at 3 months.
Doses used in major contemporary trials and what they showed:
- VITAL trial (2019, NEJM). 2,000 IU/day cholecalciferol for ~5.3 years in 25,871 US adults. No effect on the primary endpoints of invasive cancer or major cardiovascular events. Secondary signals for cancer mortality and autoimmune disease have been re-examined in extended follow-up.
- VITAL autoimmune analysis (2022). The same cohort, with autoimmune disease incidence as a pre-specified secondary endpoint, showed a 22% reduction in confirmed autoimmune disease in the vitamin D arm over five years.
- D2d (Vitamin D and Type 2 Diabetes, 2019). 4,000 IU/day for ~2.5 years in adults with prediabetes. Did not significantly prevent progression to diabetes in the overall population, with a possible signal in the subgroup that achieved 25(OH)D above 40 ng/mL.
- Martineau et al. (2017, BMJ). Individual-patient-data meta-analysis of 25 RCTs (10,933 participants) of vitamin D supplementation for prevention of acute respiratory tract infections. A protective effect was seen overall (modest), strongest in daily or weekly dosing (versus bolus doses) and in adults starting below 25 nmol/L (10 ng/mL).
- Jolliffe et al. (2021). Updated meta-analysis (43 RCTs, 48,488 participants) confirming a small protective effect of vitamin D supplementation against acute respiratory infections, with greater effect at daily 400–1,000 IU dosing.
Practical translation:
- For a generally healthy adult with no risk factors and reasonable summer sun exposure, the IOM 600–800 IU/day floor is enough to keep most people above the 20 ng/mL adequacy threshold most of the year.
- For adults with one or more risk factors (latitude, indoor lifestyle, dark skin, BMI ≥30, age 65+, malabsorption, routine sunscreen), 1,000–2,000 IU/day of cholecalciferol (D3) is a defensible default.
- Treatment of confirmed deficiency should be clinician-led; the loading-plus-maintenance approach above is the most common 2026 pattern.
- Bolus dosing (single doses of 50,000+ IU monthly or less often) has been associated with worse infection-prevention outcomes than daily dosing and is generally being phased out of guidelines.
A reminder on units: 40 IU equals 1 microgram (mcg). A 1,000 IU softgel contains 25 mcg of cholecalciferol. Labels in 2026 are required to display mcg in the US but most consumer products list both.
Vitamin D Benefits for Immunity: What 2026 Evidence Actually Supports
Vitamin D benefits for immunity is the category where the 2026 evidence base is the strongest it has ever been but is still much narrower than the consumer narrative suggests. The clearest claims that survive scrutiny are about respiratory infection risk in deficient adults and about autoimmune disease incidence at the population level. Broader claims (catches every cold, prevents the flu, treats COVID-19) are not supported by the trial evidence.
The mechanistic basis is real and well-characterized:
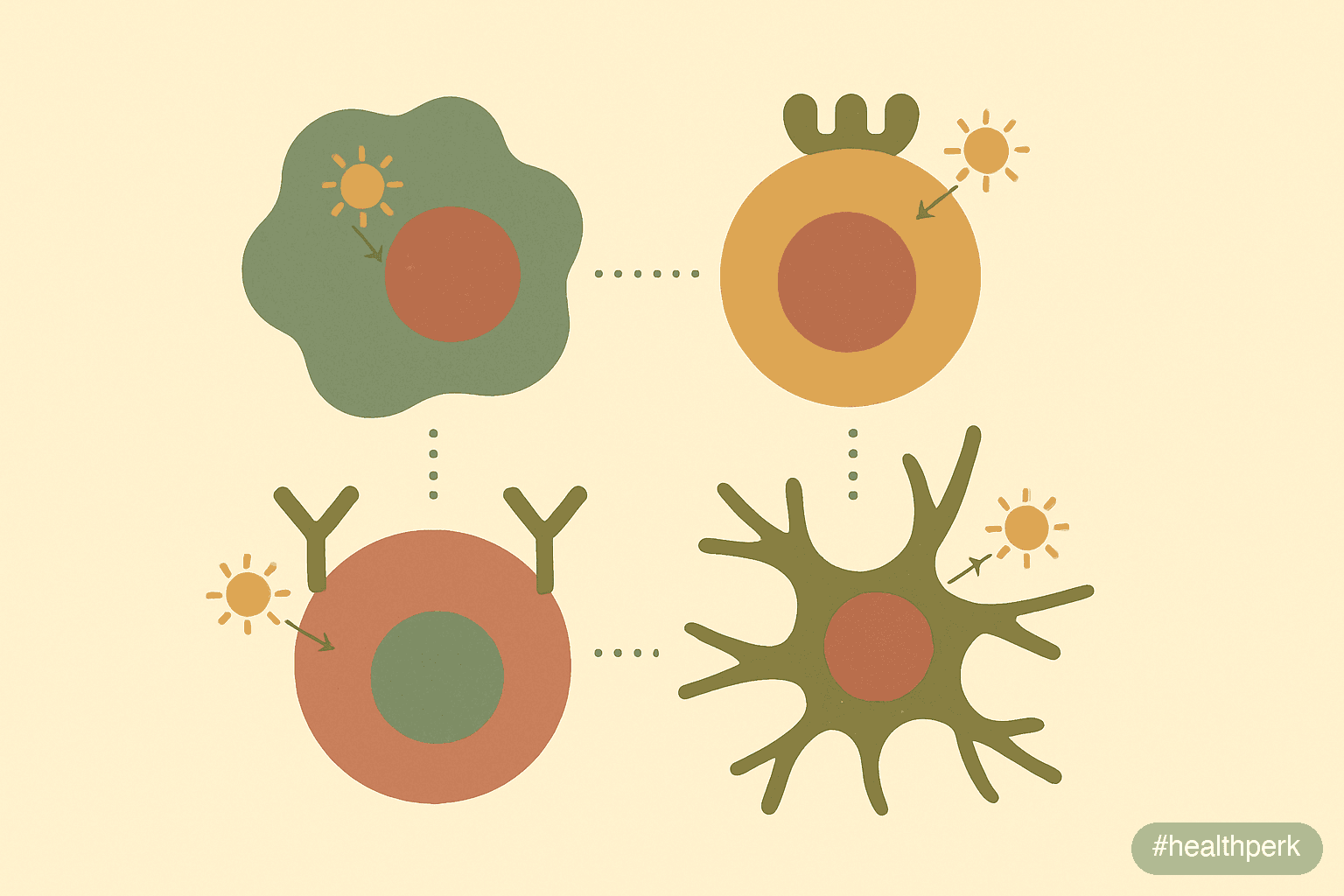
- The vitamin D receptor (VDR) is expressed on macrophages, monocytes, dendritic cells, T cells, and B cells. Activated calcitriol modulates the transcription of innate and adaptive immune genes.
- Calcitriol upregulates cathelicidin and β-defensin 2, two antimicrobial peptides produced by macrophages and epithelial cells that disrupt bacterial, fungal, and some viral membranes.
- Calcitriol promotes a shift from pro-inflammatory Th1/Th17 toward regulatory T cell phenotypes, which is the biological rationale for the autoimmune signal in trials.
- The active hormone supports tight junction integrity in respiratory epithelium, which is relevant to barrier defense against airborne pathogens.
What the clinical trial evidence supports as of 2026:
- Acute respiratory tract infections. The 2017 individual-patient-data meta-analysis and the 2021 Jolliffe update both find a small but real reduction in risk of acute respiratory infections with daily or weekly vitamin D supplementation. The protective effect is consistent but modest at the population level — number-needed-to-treat in the range of 30–80 depending on baseline status — and concentrated in adults who started below the 25 nmol/L (10 ng/mL) threshold.
- Autoimmune disease. VITAL extended follow-up showed a reduction in confirmed autoimmune disease in the supplementation arm. The absolute effect was small (about 0.5 fewer cases per 100 person-years) but reproducible across rheumatoid arthritis, autoimmune thyroid, and psoriasis.
- Tuberculosis (in deficient adults in endemic areas). Adjunctive vitamin D in confirmed pulmonary TB has shown faster sputum culture conversion in adults with specific VDR polymorphisms, particularly in trials from the UK and South Asia. This is a clinical context, not a general-population recommendation.
What the trial evidence does not support:
- Preventing or treating COVID-19 at routine supplementation doses in adults with adequate vitamin D status. Large trials (CORONAVIT, COVIT-TRIAL) found no significant effect of vitamin D on COVID-19 incidence or severity in the overall population. Observational signals were not reproduced in randomized data.
- Preventing influenza specifically. The respiratory-infection signal is non-specific and modest; the influenza-specific signal in trials has been inconsistent.
- "Boosting" immunity in adults who are already replete. The protective effect of supplementation is concentrated in adults starting from low status; above 30 ng/mL, additional supplementation does not produce a measurable further reduction in infection risk.
Practical translation: vitamin D supplementation in adults with insufficient or deficient 25(OH)D is one of the better-supported nutritional interventions for general infection resistance. Vitamin D supplementation in adults who are already replete is largely insurance against future seasonal dips rather than an active immune intervention. The right question is "what is my status" before "what dose should I take".
Do I Need Vitamin D Supplements? A Decision Framework Based on Sun, Skin, and Latitude
Do I need vitamin D supplements is one of the few supplement questions in 2026 that has a defensible structured answer. Vitamin D status is unusually individual: two adults of the same age and weight, with the same diet, can sit a full 20 ng/mL apart on serum 25(OH)D depending on their latitude, skin, and lifestyle. The honest answer is "test first, then decide" — but if testing is not accessible, a structured estimate is reasonable.
Daily vitamin D supplementation is likely useful if:
- You live above roughly 35° latitude (most of the continental US, all of Canada, almost all of Europe) and spend October through March mostly indoors. UVB is too oblique at these latitudes in winter to drive cutaneous synthesis regardless of how much daylight reaches the ground.
- You have a darker skin tone (Fitzpatrick V or VI). Melanin attenuates UVB penetration and reduces cutaneous vitamin D synthesis by a factor of three to five at any given exposure.
- You routinely use sunscreen (SPF 15+) on most exposed skin during the warm months. Sunscreen is appropriately recommended for skin cancer prevention; the trade-off is reduced vitamin D synthesis.
- You are 65 or older. Cutaneous synthesis declines with age, partly because 7-dehydrocholesterol in the skin decreases.
- Your BMI is 30 or higher. Vitamin D sequesters in adipose tissue, lowering circulating 25(OH)D at any given intake.
- You spend most daylight hours indoors (office worker, remote worker, shift worker).
- You follow a vegan or strict plant-based diet without fortified foods. Dietary vitamin D sources are concentrated in fatty fish, eggs, and fortified dairy or plant milks; cholecalciferol from lichen is the practical D3 option for vegans in 2026.
- You have a confirmed condition affecting gut fat absorption: celiac disease, Crohn's disease, post-gastric-bypass, chronic pancreatitis, cystic fibrosis.
- You have osteoporosis, osteopenia, or chronic kidney disease — supplementation should be clinician-directed in these cases.
Daily vitamin D supplementation is probably unnecessary if:
- You live below about 35° latitude and spend 15–30 minutes of midday sun on bare arms and face most days of the year.
- You have a fair-to-medium skin tone, no sunscreen-on-all-exposed-skin habit, and routinely eat fatty fish (salmon, sardines, mackerel) two to three times a week.
- You have a recent 25(OH)D test above 30 ng/mL and your circumstances have not changed.
Vitamin D supplementation needs clinician oversight if:
- You have chronic kidney disease — both 25(OH)D and active vitamin D analogs may be involved, and dosing is condition-specific.
- You have a history of nephrolithiasis (kidney stones), hyperparathyroidism, or sarcoidosis (sarcoidosis causes extrarenal activation of calcitriol and can produce hypercalcemia at modest vitamin D intakes).
- You are pregnant — 600 IU/day RDA is generally safe and many obstetric guidelines suggest 1,000–2,000 IU/day, but it is worth confirming with prenatal care.
- You are already taking other vitamin D-containing products (multivitamins, prenatal vitamins, fortified meal replacements). Stacking these can quietly push intake above the UL.
A defensible default for an adult in the "likely useful" group: 1,000–2,000 IU/day of cholecalciferol (D3) taken with the largest fat-containing meal of the day, year-round or at minimum October through April in temperate latitudes. Recheck 25(OH)D after 8–12 weeks. Adjust dose to land in the 30–50 ng/mL range; doses much higher than 4,000 IU/day are unnecessary for most adults and should be clinician-supervised.
Side effects to expect from honest dosing: none in most adults. Vitamin D toxicity (hypercalcemia, polyuria, nausea, kidney stones, in extreme cases nephrocalcinosis) generally requires sustained intake well above 10,000 IU/day for months, or a single massive bolus. The 4,000 IU/day Upper Limit is set with substantial safety margin and should not be exceeded routinely without clinician oversight.
Related Articles on HealthPerk
Explore more on this topic:
- How to Choose Supplements Safely
- Supplement Routine for Beginners
- Can You Take Multiple Supplements Together?
- Magnesium Benefits for Sleep and Anxiety
- Omega 3 Benefits for Brain Health
- Best Supplements for Immune System
Frequently Asked Questions
What are the main vitamin D deficiency symptoms?
The most reproducible signs in adults are persistent fatigue out of proportion to sleep, diffuse musculoskeletal aches (lower back, hips, shins), proximal muscle weakness noticed when climbing stairs or rising from a chair, low mood and lower stress tolerance through winter, more-frequent upper-respiratory infections than peers, slower wound healing, and — at lower thresholds — bone pain or stress fractures. Symptoms overlap heavily with sleep debt, stress, and hypothyroidism, so the only reliable confirmation is a serum 25-hydroxyvitamin D blood test, ideally drawn at the end of winter when status is at its annual nadir.
What does vitamin D actually do in the body?
Vitamin D is a secosteroid hormone, not a classical vitamin. It is synthesized in the skin from 7-dehydrocholesterol when UVB strikes the epidermis, hydroxylated in the liver to 25-hydroxyvitamin D (the storage form measured in blood), and converted in the kidney to calcitriol, the active form. Calcitriol binds the vitamin D receptor in nearly every tissue and regulates calcium absorption and bone mineralization, immune modulation through cathelicidin and T cell phenotype, muscle fiber function, and gene expression across hundreds of target genes.
What are the most common low vitamin D symptoms in adults?
Low vitamin D in adults typically presents as a cluster: persistent fatigue, diffuse musculoskeletal aches in the lower back, hips, and shins, proximal muscle weakness (harder time on stairs or rising from a chair), bone tenderness on firm pressure to the sternum or tibia, low mood worsening through winter, more-frequent colds, and slower wound healing. None of these is individually specific; the combination plus a 25(OH)D below 20 ng/mL is what makes the diagnosis. Severe and prolonged deficiency leads to osteomalacia with frank bone pain and stress-fracture risk.
How much vitamin D per day should an adult take?
The US Institute of Medicine RDA is 600 IU/day for adults 19–70 and 800 IU/day for adults 71+, with a Tolerable Upper Intake Level of 4,000 IU/day without medical oversight. The Endocrine Society 2024 guideline suggests 1,500–2,000 IU/day for adults at risk of deficiency (older adults, dark skin, limited sun, obesity, malabsorption). For most adults in temperate latitudes with one or more risk factors, 1,000–2,000 IU/day of cholecalciferol (D3) taken with a fat-containing meal is a defensible default; treatment of confirmed deficiency should be clinician-directed.
What are the vitamin D benefits for immunity in 2026?
The strongest 2026 evidence is for two outcomes: a modest reduction in acute respiratory tract infection risk (Jolliffe meta-analysis of 43 RCTs, strongest in adults starting below 25 nmol/L on daily or weekly dosing), and a reduction in autoimmune disease incidence (VITAL extended follow-up, 22% relative reduction over five years). The trial evidence does not support routine vitamin D supplementation for prevention or treatment of COVID-19 in adults with adequate status, and the broader "boost immunity" claim is not supported in adults who are already replete above 30 ng/mL.
Do I need vitamin D supplements?
Likely yes if you live above 35° latitude with mostly indoor winters, have darker skin (Fitzpatrick V or VI), routinely use sunscreen on all exposed skin, are 65+, have a BMI of 30 or higher, eat little fatty fish, follow a strict plant-based diet, or have a malabsorption condition. Probably no if you live in a sunny latitude with daily midday sun on bare skin and eat fatty fish two to three times a week. Clinician oversight is needed in chronic kidney disease, sarcoidosis, primary hyperparathyroidism, kidney stone history, or pregnancy. The honest answer is to test 25(OH)D first.
What 25-hydroxyvitamin D level is considered adequate?
The Institute of Medicine defines below 12 ng/mL (30 nmol/L) as deficient, 12–20 ng/mL as insufficient, and 20–50 ng/mL as adequate for general population bone health. The Endocrine Society defines 30–50 ng/mL (75–125 nmol/L) as the target for clinical patients at risk. Levels above 50 ng/mL are not associated with additional benefit and levels above 100 ng/mL begin to raise concern for excessive intake. The most defensible target for adults in 2026 is 30–50 ng/mL, retested annually if supplementing.
Can vitamin D supplements interact with my medications?
Yes. Vitamin D absorption can be reduced by long-term use of orlistat, cholestyramine, mineral oil, and other fat-blocking agents. Anticonvulsants (phenytoin, phenobarbital, carbamazepine), oral corticosteroids, and certain antiretrovirals accelerate vitamin D catabolism and may require higher maintenance doses. Adults with chronic kidney disease, primary hyperparathyroidism, sarcoidosis, or a history of kidney stones should not start routine vitamin D supplementation without clinician oversight, because abnormal calcium handling can produce hypercalcemia at modest vitamin D intakes.
This article is for informational purposes only and does not constitute medical advice. Vitamin D supplementation requires clinician oversight in adults with chronic kidney disease, primary hyperparathyroidism, sarcoidosis, a history of kidney stones, or hypercalcemia, and during pregnancy and lactation. Adults on anticonvulsants, oral corticosteroids, or antiretrovirals may need adjusted dosing. Self-treatment of suspected deficiency above 4,000 IU/day or self-dosed loading regimens are not recommended without a confirmed 25(OH)D measurement. Individual results may vary.
About the author The HealthPerk Editorial Team reviews nutritional and supplement research through evidence synthesis cross-referenced with peer-reviewed clinical trials, Cochrane reviews, and clinical practice guidelines. Our supplement content is reviewed for medical accuracy against current internal medicine and nutritional science standards. How we review →
References
Office of Dietary Supplements, National Institutes of Health. (2024). Vitamin D: Fact Sheet for Health Professionals. U.S. Department of Health and Human Services. https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/
Supports: RDA values, Tolerable Upper Intake Level, deficiency thresholds, NHANES prevalence estimates, and risk groups
Institute of Medicine. (2011). Dietary Reference Intakes for Calcium and Vitamin D. National Academies Press. https://doi.org/10.17226/13050
Supports: 600–800 IU/day RDA basis, 4,000 IU/day Tolerable Upper Intake Level, and 20 ng/mL adequacy threshold
Demay, M. B., Pittas, A. G., Bikle, D. D., Diab, D. L., Kiely, M. E., Lazaretti-Castro, M., ... & Sempos, C. T. (2024). Vitamin D for the prevention of disease: An Endocrine Society clinical practice guideline. Journal of Clinical Endocrinology & Metabolism, 109(8), 1907–1947. https://doi.org/10.1210/clinem/dgae290
Supports: 2024 Endocrine Society dosing guidance for at-risk adults, 30 ng/mL clinical target, loading-plus-maintenance approach
Martineau, A. R., Jolliffe, D. A., Hooper, R. L., Greenberg, L., Aloia, J. F., Bergman, P., ... & Camargo, C. A. (2017). Vitamin D supplementation to prevent acute respiratory tract infections: Systematic review and meta-analysis of individual participant data. BMJ, 356, i6583. https://doi.org/10.1136/bmj.i6583
Supports: individual-patient-data meta-analysis showing modest protective effect on acute respiratory infections, strongest with daily/weekly dosing and lower baseline 25(OH)D
Jolliffe, D. A., Camargo, C. A., Sluyter, J. D., Aglipay, M., Aloia, J. F., Ganmaa, D., ... & Martineau, A. R. (2021). Vitamin D supplementation to prevent acute respiratory infections: A systematic review and meta-analysis of aggregate data from randomised controlled trials. Lancet Diabetes & Endocrinology, 9(5), 276–292. https://doi.org/10.1016/S2213-8587(21)00051-6
Supports: updated 43-trial meta-analysis confirming small protective effect at daily 400–1,000 IU dosing
Manson, J. E., Cook, N. R., Lee, I. M., Christen, W., Bassuk, S. S., Mora, S., ... & Buring, J. E. (2019). Vitamin D supplements and prevention of cancer and cardiovascular disease. New England Journal of Medicine, 380(1), 33–44. https://doi.org/10.1056/NEJMoa1809944
Supports: VITAL primary endpoint findings — no effect of 2,000 IU/day cholecalciferol on cancer or cardiovascular endpoints over 5.3 years
Hahn, J., Cook, N. R., Alexander, E. K., Friedman, S., Walter, J., Bubes, V., ... & Costenbader, K. H. (2022). Vitamin D and marine omega 3 fatty acid supplementation and incident autoimmune disease: VITAL randomized controlled trial. BMJ, 376, e066452. https://doi.org/10.1136/bmj-2021-066452
Supports: 22% reduction in confirmed autoimmune disease in the vitamin D arm of VITAL over five years
Pittas, A. G., Dawson-Hughes, B., Sheehan, P., Ware, J. H., Knowler, W. C., Aroda, V. R., ... & Hu, F. B. (2019). Vitamin D supplementation and prevention of type 2 diabetes. New England Journal of Medicine, 381(6), 520–530. https://doi.org/10.1056/NEJMoa1900906
Supports: D2d trial — 4,000 IU/day did not significantly prevent progression to type 2 diabetes overall, with subgroup signal at higher achieved 25(OH)D
Holick, M. F. (2007). Vitamin D deficiency. New England Journal of Medicine, 357(3), 266–281. https://doi.org/10.1056/NEJMra070553
Supports: foundational review of vitamin D physiology, cutaneous synthesis, hydroxylation pathway, and clinical features of deficiency
Bouillon, R., Manousaki, D., Rosen, C., Trajanoska, K., Rivadeneira, F., & Richards, J. B. (2022). The health effects of vitamin D supplementation: Evidence from human studies. Nature Reviews Endocrinology, 18(2), 96–110. https://doi.org/10.1038/s41574-021-00593-z
Supports: 2022 evidence synthesis on vitamin D supplementation effects, including immune, autoimmune, and musculoskeletal endpoints
Frequently Asked Questions
What are the main vitamin D deficiency symptoms?
The most reproducible signs in adults are persistent fatigue out of proportion to sleep, diffuse musculoskeletal aches (lower back, hips, shins), proximal muscle weakness noticed when climbing stairs or rising from a chair, low mood and lower stress tolerance through winter, more-frequent upper-respiratory infections than peers, slower wound healing, and - at lower thresholds - bone pain or stress fractures. Symptoms overlap heavily with sleep debt, stress, and hypothyroidism, so the only reliable confirmation is a serum 25-hydroxyvitamin D blood test, ideally drawn at the end of winter when status is at its annual nadir.
What does vitamin D actually do in the body?
Vitamin D is a secosteroid hormone, not a classical vitamin. It is synthesized in the skin from 7-dehydrocholesterol when UVB strikes the epidermis, hydroxylated in the liver to 25-hydroxyvitamin D (the storage form measured in blood), and converted in the kidney to calcitriol, the active form. Calcitriol binds the vitamin D receptor in nearly every tissue and regulates calcium absorption and bone mineralization, immune modulation through cathelicidin and T cell phenotype, muscle fiber function, and gene expression across hundreds of target genes.
What are the most common low vitamin D symptoms in adults?
Low vitamin D in adults typically presents as a cluster: persistent fatigue, diffuse musculoskeletal aches in the lower back, hips, and shins, proximal muscle weakness (harder time on stairs or rising from a chair), bone tenderness on firm pressure to the sternum or tibia, low mood worsening through winter, more-frequent colds, and slower wound healing. None of these is individually specific; the combination plus a 25(OH)D below 20 ng/mL is what makes the diagnosis. Severe and prolonged deficiency leads to osteomalacia with frank bone pain and stress-fracture risk.
How much vitamin D per day should an adult take?
The US Institute of Medicine RDA is 600 IU/day for adults 19-70 and 800 IU/day for adults 71+, with a Tolerable Upper Intake Level of 4,000 IU/day without medical oversight. The Endocrine Society 2024 guideline suggests 1,500-2,000 IU/day for adults at risk of deficiency (older adults, dark skin, limited sun, obesity, malabsorption). For most adults in temperate latitudes with one or more risk factors, 1,000-2,000 IU/day of cholecalciferol (D3) taken with a fat-containing meal is a defensible default; treatment of confirmed deficiency should be clinician-directed.
What are the vitamin D benefits for immunity in 2026?
The strongest 2026 evidence is for two outcomes: a modest reduction in acute respiratory tract infection risk (Jolliffe meta-analysis of 43 RCTs, strongest in adults starting below 25 nmol/L on daily or weekly dosing), and a reduction in autoimmune disease incidence (VITAL extended follow-up, 22% relative reduction over five years). The trial evidence does not support routine vitamin D supplementation for prevention or treatment of COVID-19 in adults with adequate status, and the broader boost immunity claim is not supported in adults who are already replete above 30 ng/mL.
Do I need vitamin D supplements?
Likely yes if you live above 35 degrees latitude with mostly indoor winters, have darker skin (Fitzpatrick V or VI), routinely use sunscreen on all exposed skin, are 65+, have a BMI of 30 or higher, eat little fatty fish, follow a strict plant-based diet, or have a malabsorption condition. Probably no if you live in a sunny latitude with daily midday sun on bare skin and eat fatty fish two to three times a week. Clinician oversight is needed in chronic kidney disease, sarcoidosis, primary hyperparathyroidism, kidney stone history, or pregnancy. The honest answer is to test 25(OH)D first.
What 25-hydroxyvitamin D level is considered adequate?
The Institute of Medicine defines below 12 ng/mL (30 nmol/L) as deficient, 12-20 ng/mL as insufficient, and 20-50 ng/mL as adequate for general population bone health. The Endocrine Society defines 30-50 ng/mL (75-125 nmol/L) as the target for clinical patients at risk. Levels above 50 ng/mL are not associated with additional benefit and levels above 100 ng/mL begin to raise concern for excessive intake. The most defensible target for adults in 2026 is 30-50 ng/mL, retested annually if supplementing.
Can vitamin D supplements interact with my medications?
Yes. Vitamin D absorption can be reduced by long-term use of orlistat, cholestyramine, mineral oil, and other fat-blocking agents. Anticonvulsants (phenytoin, phenobarbital, carbamazepine), oral corticosteroids, and certain antiretrovirals accelerate vitamin D catabolism and may require higher maintenance doses. Adults with chronic kidney disease, primary hyperparathyroidism, sarcoidosis, or a history of kidney stones should not start routine vitamin D supplementation without clinician oversight, because abnormal calcium handling can produce hypercalcemia at modest vitamin D intakes.
More from Supplements


