
Why Can't I Lose Weight Even Dieting? An Evidence-Based Guide to Stalled Fat Loss
Why Can't I Lose Weight Even Dieting? An Evidence-Based Guide to Stalled Fat Loss
By the HealthPerk Editorial Team · Last updated: May 2026
Quick Answer
Why can't I lose weight even when I am dieting?
In most adults who feel stuck, the cause is one of four overlapping factors: a deficit that exists on paper but not in practice (under-reported intake plus over-reported activity), metabolic adaptation that has shrunk the effective deficit, recovery deficits in sleep and stress that elevate cortisol and appetite hormones, or normal short-term fluctuations from water, glycogen, and hormonal cycling that mask underlying fat loss. The pattern matters more than any single number — fat loss is a multi-week trend, not a daily readout.
Match the pattern to the most likely driver:
| If the stall feels like… | Most likely driver | First step |
|---|---|---|
| Scale frozen for 2–3 weeks despite identical eating | Metabolic adaptation + accumulated water retention | Diet break for 1–2 weeks at maintenance, then resume |
| Weight up after a stressful week of identical eating | Cortisol-driven water retention, not fat gain | Sleep recovery, slower waist measurements, ignore daily scale |
| Hungry constantly, snacking creeping back in | Under-reported intake from portion drift | One week of measured weighing, not estimating |
| Workouts feel hard, mood is flat, sleep is poor | Aggressive deficit + recovery debt | Raise calories 10–15%, prioritize sleep regularity |
The experience of dieting carefully and seeing no movement on the scale is one of the most common and discouraging patterns in weight management. Why can't I lose weight even dieting is rarely answered by a single cause — it is the intersection of biological adaptation, behavioral drift, recovery deficits, and the lagging signal-to-noise of body composition itself. The encouraging implication is that almost every plateau has an identifiable cause, and most resolve within 2–4 weeks once the right lever is moved.
By 2026, the consensus across obesity medicine, behavioral science, and metabolic research has converged on a more nuanced view than the simple "calories in, calories out" framing of a decade ago. The energy balance equation still holds — fat loss requires a net energy deficit — but every term in the equation is dynamic. Intake estimates drift, activity contracts as weight drops, resting metabolic rate adapts, and recovery deficits change the appetite signals that determine adherence. The honest answer to "why is the scale not moving" almost always lies in one of those moving terms.
This guide maps the most common drivers of stalled fat loss with the strongest 2026 evidence, organized by leverage rather than novelty.
Table of Contents
- Why Am I Not Losing Weight in a Calorie Deficit
- Weight Loss Plateau: What to Do
- How to Break a Weight Loss Plateau
- Why Do I Gain Weight Easily
- Sleep and Weight Loss Connection
- Stress and Weight Gain
- Habits for Weight Loss Success
- How to Lose Weight Sustainably
- Frequently Asked Questions
- References
Why Am I Not Losing Weight in a Calorie Deficit
The question why am I not losing weight in a calorie deficit has three honest answers that account for the vast majority of cases, before any rare metabolic pathology should be considered.
The first is that the deficit on paper is not the deficit in practice. A frequently cited 1992 New England Journal of Medicine study by Lichtman and colleagues found that adults with a history of diet-resistance under-reported their food intake by an average of 47% and over-reported physical activity by 51% when intake was measured by doubly-labeled water (Lichtman et al., 1992). The effect is not lying — it is cognitive estimation drift, and it occurs in trained nutrition professionals as well as lay dieters. Tracking apps inherit the same error: portion sizes are estimated, labels carry ±20% tolerances, and oils and condiments are often invisible in the count.
The second is that the deficit was real but has shrunk through metabolic adaptation. As body mass falls, resting metabolic rate falls in rough proportion, and non-exercise activity thermogenesis (NEAT) often contracts as the body conserves energy. A 2016 Obesity study following participants from "The Biggest Loser" documented metabolic adaptation persisting six years after rapid weight loss, with measured resting metabolism running 500 kcal/day below predicted (Fothergill et al., 2016). The effect is most pronounced after aggressive, rapid loss; it is smaller but still meaningful after moderate loss.
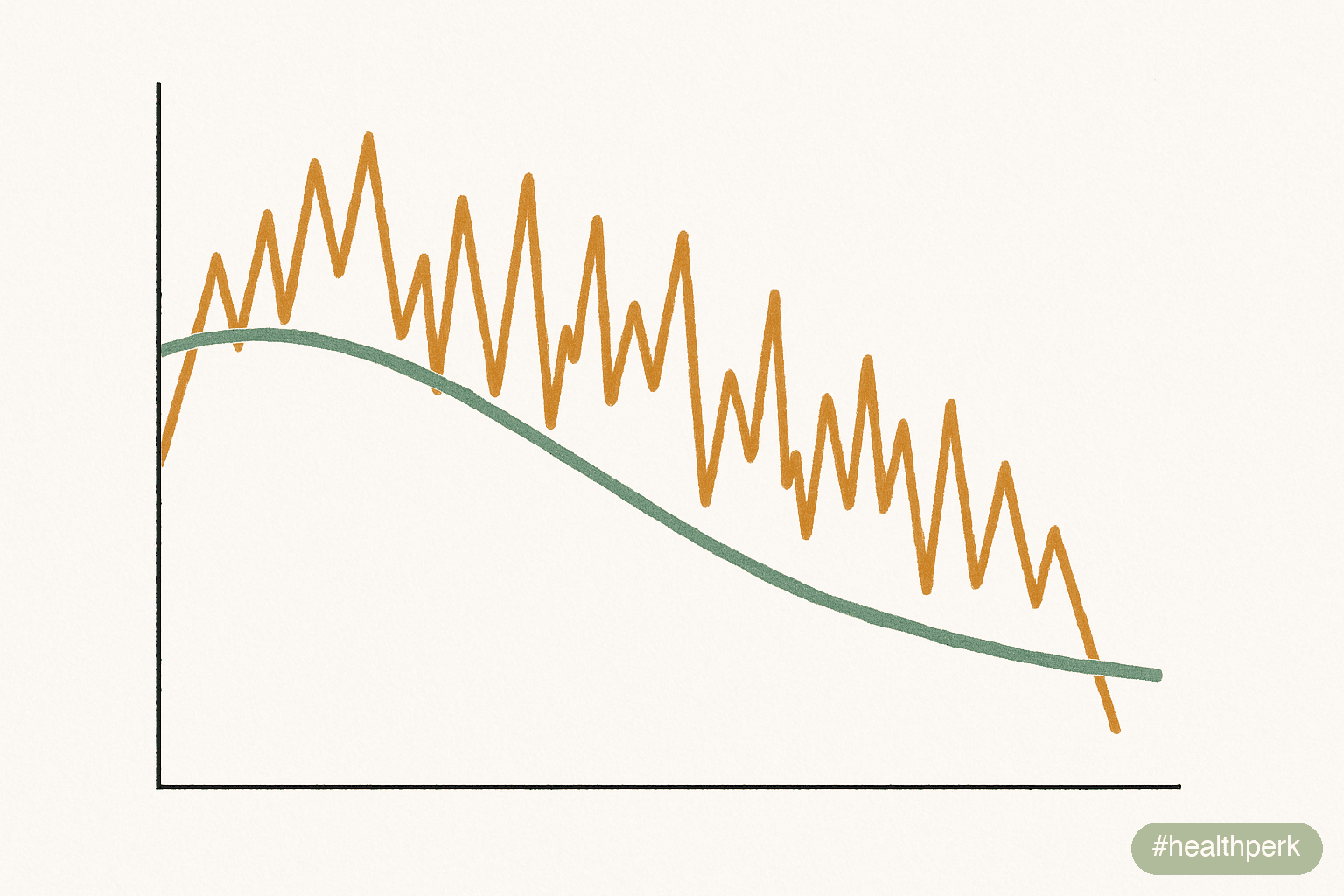
The third is that fat loss is occurring but is masked by water, glycogen, and digestive-content fluctuation. Each gram of glycogen carries 3–4 grams of water; each gram of sodium retains ~10 ml of water; menstrual-cycle hormones shift water by 1–3 lb across a month; and stress, travel, or unfamiliar food can swing weight by similar amounts within 24 hours. A scale that has not moved in 10 days may be tracking a real loss buried under retained water.
The practical diagnostic: measure for one week with a kitchen scale and a paper log, weigh daily under standardized conditions (after waking, after the bathroom, before food or water), and use the weekly average as the signal. If the weekly average has not dropped for three consecutive weeks at a logged 500 kcal/day deficit, adaptation or measurement drift is the most likely cause.
Weight Loss Plateau: What to Do
Weight loss plateau what to do is the most-searched follow-up to "why is the scale not moving," and the answer is sequential rather than additive. Most plateaus are not plateaus at all — they are 2–3 week stretches of normal noise that look like a stall when viewed as a daily line. The first step is to confirm a plateau exists.
A genuine plateau is defined as three or more consecutive weeks of no movement in the weekly weight average at a logged deficit, not a single flat week. Anything shorter is statistical noise — body weight has a normal day-to-day standard deviation of roughly 1–3 lb from glycogen, sodium, and bowel content alone, and a 7-day average can stay flat across two weeks while underlying fat loss continues.
Once a plateau is confirmed at the three-week mark, the order of operations is:
- Audit intake for one week. Weigh everything in grams on a kitchen scale, including oils, dressings, and bites-while-cooking. Do not change anything else. Most plateaus resolve at this step — actual intake was 200–400 kcal/day above estimated.
- Audit activity. Step counts often quietly drop 1,500–3,000 steps as diet fatigue accumulates. NEAT contraction is real and significant. If steps have dropped, restore them before cutting calories further.
- Take a 1–2 week diet break at maintenance. A 2017 International Journal of Obesity trial (MATADOR) showed intermittent calorie restriction with two-week breaks at maintenance produced superior fat loss and less metabolic adaptation than continuous restriction (Byrne et al., 2018).
- Only then, after audit and a break, reduce calories or increase activity by ~10–15%. Aggressive cuts shorten the runway and worsen adaptation.
The temptation under a plateau is to cut harder. The evidence supports the opposite: audit first, recover second, and only then re-deepen the deficit modestly.
How to Break a Weight Loss Plateau
How to break a weight loss plateau depends on which of the three underlying drivers (estimation drift, adaptation, water masking) is dominant. The audit step in the prior section diagnoses which driver is in play; the corrective levers differ by driver.
If estimation drift is dominant — actual intake exceeded planned intake during the audit week — the lever is precision, not restriction. Returning to weighed portions for 1–2 weeks restores the deficit without cutting it.
If adaptation is dominant — intake was accurate, activity preserved, and weekly average truly flat across 3+ weeks — the strongest 2026-supported intervention is a structured diet break. The MATADOR trial cited above and a 2014 European Group on Obesity meta-review converged on the same finding: planned interruptions to caloric restriction reduce metabolic adaptation and improve total fat loss compared with continuous restriction of equal duration. Practical protocol: 1–2 weeks eating at calculated maintenance (current weight × 14–15 kcal/lb for moderately active), with protein held constant at 0.7–1.0 g/lb, then resume the deficit. Most people see weight resume falling within the first week after the break.
If water masking is dominant — measurements such as waist circumference, progress photos, or strength performance show change while the scale does not — the corrective lever is patience plus salt and stress audit. Reducing sodium variability, restoring sleep, and continuing the protocol typically reveals a 2–4 lb whoosh within 7–10 days.
What does not work, by 2026 evidence: extreme calorie cuts (under 1,200 kcal/day in women, 1,500 kcal/day in men) worsen adaptation without faster loss; cardio-on-cardio "burning more" rarely outpaces the appetite increase it generates; and changing macronutrient ratios without changing total intake produces water and glycogen shifts that look like fat loss but rarely are.
Refeeds and reverse dieting
A planned high-carbohydrate refeed day (1–2 days at maintenance, with carbohydrates emphasized) can restore leptin and thyroid hormone signaling and improve adherence the following week. The evidence base for refeeds is smaller than for full diet breaks, but they are a useful tool inside longer diets when a full 1–2 week break is not feasible.
Why Do I Gain Weight Easily

Why do I gain weight easily is a question about both biology and behavior, and the honest answer involves both. Some adults do have biological set points and energy economics that make weight regain more rapid for the same nutritional environment — but the variance is smaller than commonly assumed and behavioral factors usually dominate.
The biological contributors that have the strongest evidence in 2026:
- History of weight loss. A 2011 New England Journal of Medicine study by Sumithran and colleagues followed adults one year after a 10% diet-induced weight loss and found persistent shifts in appetite hormones — lower leptin, higher ghrelin, higher hunger ratings — that persisted at 12 months and predicted regain (Sumithran et al., 2011). The body defends a previous high weight for years.
- Sleep debt. Short and irregular sleep elevates ghrelin (the hunger signal), reduces leptin (the fullness signal), and shifts food choice toward calorically dense, palatable options. The effect is measurable within a single night of restricted sleep.
- Genetic variation in fat storage and hunger signals. Modest contributions from FTO, MC4R, and related loci affect appetite and adiposity, though they are smaller than environmental and behavioral effects in most populations.
Gaining weight without eating more
Gaining weight without eating more is a real and frustrating experience, and the explanations are usually mundane rather than mysterious. The most common are:
- NEAT contraction. Day-to-day movement (fidgeting, standing, walking) can vary by 1,500–2,000 kcal between high- and low-NEAT days. A new desk job, an injury, or even a stressful week can quietly reduce daily expenditure without any change in formal exercise.
- Sleep deprivation increasing appetite hormones, which then increases intake in ways that often escape conscious tracking — late-evening snacking, larger pours of olive oil, second helpings.
- Medications. Several common classes — some antidepressants, antipsychotics, beta-blockers, corticosteroids, insulin, certain hormonal contraceptives — produce real weight gain independent of intake. If timing matches a medication change, the prescriber should be consulted.
- Endocrine causes, particularly hypothyroidism and Cushing's syndrome. These are less common but worth ruling out with a single blood panel if weight gain is rapid (>5 lb/month unexplained) or accompanied by other symptoms.
- Fluid retention from sodium, premenstrual hormones, alcohol, or new medications. Often resolves within 7–14 days.
The behavioral check that resolves most cases: weigh food in grams for one week without changing anything else. Reported intake tends to converge with measured intake within 200–400 kcal/day.
Sleep and Weight Loss Connection
The sleep and weight loss connection is one of the most under-leveraged variables in weight management. A 2010 Annals of Internal Medicine trial by Nedeltcheva and colleagues randomized adults on identical calorie-restricted diets to either 5.5 or 8.5 hours of sleep nightly; the shorter sleepers lost 55% less fat and 60% more lean mass over two weeks (Nedeltcheva et al., 2010). The deficit was identical — the body composition outcome was not.
A 2022 JAMA Internal Medicine trial extended this further, showing that simply increasing sleep duration in habitually short-sleeping adults reduced spontaneous energy intake by ~270 kcal/day, without any conscious diet intervention (Tasali et al., 2022). Sleep is among the few interventions that reduces intake without willpower.
Mechanisms with the strongest evidence:
- Short sleep elevates ghrelin and reduces leptin, shifting hunger and satiety toward overconsumption
- Fragmented sleep impairs glucose tolerance and increases insulin resistance, biasing energy toward fat storage
- Sleep deprivation reduces NEAT and exercise adherence the following day
- Late-evening sleep timing shifts melatonin into the eating window, worsening glucose handling for late meals
Practical levers, in order of effect:
- Fix wake time first. A 30-minute weekend window; consistency outranks duration.
- 10 minutes of outdoor daylight within 30 minutes of waking. Anchors circadian phase.
- Cap caffeine at 14:00 if metabolism is slow; later caffeine fragments slow-wave sleep without subjective awareness.
- Cool, dark bedroom (16–19 °C), screens out the last 60 minutes.
- Screen for sleep apnea if snoring, witnessed pauses, or unrefreshing sleep are present.
Of all the non-dietary levers in weight management, sleep regularity has the best ratio of effect size to required effort.
Stress and Weight Gain

Stress and weight gain are linked through multiple mechanisms — hormonal, behavioral, and water-balance — and the relationship runs in both directions. Chronic stress raises cortisol, which transiently increases appetite (especially for energy-dense, palatable foods), promotes visceral fat storage in some individuals, and produces water retention that masks fat loss on the scale.
A 2017 Obesity study of more than 2,500 adults followed for four years found that those with persistently elevated hair cortisol — a long-term cortisol exposure marker — had higher BMI and waist circumference than controls, independent of diet and activity (Jackson et al., 2017). The effect is real but smaller than commonly portrayed; stress amplifies weight problems rather than creating them de novo.
Behavioral pathways are often the dominant mechanism in practice:
- Stress-driven eating ("eating to feel better") tends to favor calorically dense foods
- Stress shifts food choices toward convenience options with higher calorie density
- Stress disrupts sleep, which compounds appetite dysregulation
- Stress reduces willingness to plan, weigh, or prepare food, increasing reliance on prepared foods
Recovery interventions with the strongest evidence:
- Cyclic sighing — 2 nasal inhales, slow mouth exhale, repeated for 5 minutes. A 2023 Cell Reports Medicine trial by Balban and colleagues found cyclic sighing reduced physiological arousal and improved mood more than mindfulness meditation in the same time window (Balban et al., 2023).
- Walking outdoors, 20+ minutes daily. Reliably reduces cortisol and supports adherence.
- Maintained social contact. Brief in-person social connection lowers next-day cortisol.
- Adequate sleep, as above — stress and sleep are coupled and improve together.
The body composition payoff is rarely immediate. Cortisol-mediated water retention can mask 2–5 lb of true fat loss for weeks at a time; resolution is often a "whoosh" within 5–10 days of restored sleep and reduced acute stress.
Habits for Weight Loss Success
Habits for weight loss success are the structural choices that determine whether the protocol survives contact with a normal life. Long-term outcomes data — including the National Weight Control Registry, which has tracked 10,000+ adults who lost ≥30 lb and maintained it ≥1 year — point consistently to a small set of structural habits rather than any single dietary approach (Wing & Phelan, 2005).
The habits with the strongest evidence for both initial loss and maintenance:
- Self-weighing on a stable cadence. Daily or weekly weigh-ins, with the weekly average tracked, predicts better outcomes than no weighing or sporadic weighing. The function is informational, not punitive.
- Protein at every meal. 0.7–1.0 g/lb of body weight daily, distributed across 3–4 meals, supports satiety, lean mass preservation, and adherence.
- Consistent food log for the first 8–12 weeks. Logging fades as eating patterns stabilize, but early-phase logging predicts better outcomes.
- A target step count, not a workout-only mindset. Daily step targets (7,000–10,000 for most adults) protect NEAT, which is more variable and more impactful than formal exercise alone.
- Stable sleep timing. As above — single highest non-dietary lever.
- Plan for the meal you will skip. Most lapses occur in the meal that was not planned; defaults for the "missed" meal prevent calorie spikes.
- One scheduled higher-calorie meal weekly. A pre-planned "off-protocol" meal reduces the binge-restrict cycle without meaningfully slowing weekly progress.
A useful frame: long-term weight outcomes depend less on diet brand and more on routine architecture. People who succeed long-term have arranged their environments to require less ongoing decision-making — the kitchen is stocked with default foods, lunch is the same most weekdays, and the social calendar accommodates the protocol rather than fighting it.
How to Lose Weight Sustainably

How to lose weight sustainably is the right question, because the failure mode in weight loss is rarely the loss itself — it is regain. A 1995 review and many subsequent follow-ups have documented that 80%+ of adults regain most weight lost within 3–5 years when the loss is achieved through aggressive short-term restriction. The sustainable rate of loss and the sustainable protocol are different from the fastest possible loss.
The evidence-supported parameters of sustainable loss:
- Rate: 0.5–1.0% of body weight per week. For a 200 lb adult, 1–2 lb/week. Faster rates produce more metabolic adaptation, more lean mass loss, and lower long-term retention.
- Deficit size: 15–25% below maintenance. Larger deficits accelerate loss for a few weeks then plateau via adaptation and adherence failure.
- Protein: 0.7–1.0 g/lb body weight. Preserves lean mass during deficit.
- Resistance training: 2–3 sessions weekly. Preserves lean mass and basal metabolic rate.
- Sleep regularity, as above. Non-negotiable.
- Planned diet breaks every 6–10 weeks of continuous deficit, with 1–2 weeks at maintenance.
- A pre-defined maintenance plan, not an open-ended "I'll just eat normally" approach at the end. Most regain occurs in the first 6 months after loss; a structured transition prevents it.
Sustainable rates feel slow inside a culture that markets 10 lb/week protocols. The honest math: a 1 lb/week loss over 6 months is 26 lb; the same person attempting 3 lb/week typically loses 12 lb and regains 18 within a year. Slower wins on the timescale that matters.
The behavioral test for sustainability is simple: would you do this protocol if the scale never moved? If the answer is no, the protocol is unlikely to outlast the loss phase. The protocols people maintain are the ones that feel normal at maintenance — not punitive at deficit.
Related Articles on HealthPerk
Explore more on this topic:
- How to Boost Metabolism Naturally
- How to Lose Belly Fat Naturally
- Best Supplements for Weight Loss
- Natural Appetite Suppressants That Work
- Hormonal Weight Gain Causes
Frequently Asked Questions
Why can't I lose weight even when I'm dieting carefully?
The most common drivers are estimation drift (actual intake exceeds planned intake by 200–400 kcal/day on average), metabolic adaptation (resting metabolism and NEAT contract as weight drops), recovery deficits (short or irregular sleep elevates appetite hormones), and water masking (cortisol, sodium, and menstrual hormones shift water by several pounds for weeks). The diagnostic step is one week of weighed food intake with daily weigh-ins averaged across the week — most stalls resolve at this audit step before any biological cause needs to be considered.
Why am I not losing weight in a calorie deficit?
The honest answer is usually that the deficit is smaller in practice than on paper. Adults with a history of diet resistance under-report intake by an average of 47% and over-report activity by ~50% when measured against doubly-labeled water. Tracking apps inherit ±20% label tolerances and miss oils and condiments. The corrective is weighing food in grams for 1–2 weeks. If precision-tracked intake still produces no loss after 3 weeks, metabolic adaptation is the next likely cause, and a 1–2 week diet break at maintenance typically restores progress.
What does a real weight loss plateau look like, and what should I do?
A genuine plateau is three or more consecutive weeks with no movement in the weekly weight average at a logged deficit — not a single flat week. Daily weight has a normal noise range of 1–3 lb from glycogen, sodium, and bowel content. Once a plateau is confirmed, the order of operations is: audit intake by weighing in grams for one week, audit activity (step counts often quietly drop), take a 1–2 week diet break at maintenance, and only then reduce calories or increase activity by ~10–15%. Aggressive cuts shorten the runway and worsen adaptation.
How do I break a weight loss plateau without starving?
The strongest 2026-supported intervention is a structured 1–2 week diet break at calculated maintenance, with protein held constant. A randomized trial (MATADOR) showed intermittent restriction with two-week maintenance breaks produced more total fat loss and less metabolic adaptation than continuous restriction of the same duration. Refeeds (1–2 high-carbohydrate days at maintenance) are a smaller-effect alternative when a full break is not feasible. Cutting calories further during a plateau usually worsens adaptation and adherence without faster loss.
How does the sleep and weight loss connection affect a deficit?
Strongly. A randomized trial of adults on identical calorie-restricted diets found that the group sleeping 5.5 hours lost 55% less fat and 60% more lean mass than the group sleeping 8.5 hours over two weeks. A separate trial showed that increasing sleep duration in habitually short sleepers reduced spontaneous intake by ~270 kcal/day without any diet intervention. Sleep is one of few interventions that reduces appetite without willpower; fixing wake-time regularity is the single highest-yield non-dietary lever.
How do I lose weight sustainably without regaining it?
The evidence-supported parameters: 0.5–1.0% of body weight per week, deficit 15–25% below maintenance, protein 0.7–1.0 g/lb, resistance training 2–3× weekly, sleep regularity, planned diet breaks every 6–10 weeks, and a pre-defined maintenance plan that is not "just eat normally." Most regain occurs in the first six months after loss; a structured transition with continued self-weighing, food logging during high-risk periods, and stable habits predicts maintenance better than any specific diet pattern. The behavioral test for sustainability is whether the protocol would still feel normal at maintenance.
What habits matter most for long-term weight loss success?
The National Weight Control Registry, which tracks adults who maintained ≥30 lb of loss for ≥1 year, points consistently to a small set of structural habits: regular self-weighing with weekly averaging, protein at every meal, daily step targets that protect NEAT, stable sleep timing, an early-phase food log that fades as patterns stabilize, defaults for the meals most likely to be skipped, and a planned higher-calorie meal weekly to prevent binge-restrict cycles. The diet brand matters less than the routine architecture; people who succeed long-term have arranged environments that require less ongoing decision-making.
This article is for informational purposes only and does not constitute medical advice. Unexplained weight changes can be a symptom of treatable conditions including hypothyroidism, Cushing's syndrome, PCOS, diabetes, depression, eating disorders, and side effects of common medications. Consult a qualified healthcare provider for rapid unexplained weight change (>5 lb/month), inability to lose weight despite documented sustained caloric deficit beyond 12 weeks, or symptoms accompanying the weight change. Do not start or stop prescription medications without supervision. Individual results may vary.
About the author The HealthPerk Editorial Team reviews weight management research through evidence synthesis cross-referenced with peer-reviewed clinical trials and clinical practice guidelines. Our weight-loss content is reviewed for medical accuracy against current obesity-medicine, endocrinology, and behavioral health standards. How we review →
References
Lichtman, S. W., Pisarska, K., Berman, E. R., Pestone, M., Dowling, H., Offenbacher, E., ... & Heymsfield, S. B. (1992). Discrepancy between self-reported and actual caloric intake and exercise in obese subjects. New England Journal of Medicine, 327(27), 1893–1898. https://doi.org/10.1056/NEJM199212313272701
Supports: adults with diet resistance under-report intake by ~47% and over-report activity by ~51% when measured against doubly-labeled water
Fothergill, E., Guo, J., Howard, L., Kerns, J. C., Knuth, N. D., Brychta, R., ... & Hall, K. D. (2016). Persistent metabolic adaptation 6 years after "The Biggest Loser" competition. Obesity, 24(8), 1612–1619. https://doi.org/10.1002/oby.21538
Supports: metabolic adaptation persists years after rapid weight loss, with resting metabolism running below predicted
Byrne, N. M., Sainsbury, A., King, N. A., Hills, A. P., & Wood, R. E. (2018). Intermittent energy restriction improves weight loss efficiency in obese men: The MATADOR study. International Journal of Obesity, 42(2), 129–138. https://doi.org/10.1038/ijo.2017.206
Supports: planned diet breaks at maintenance produce more total fat loss and less metabolic adaptation than continuous restriction
Sumithran, P., Prendergast, L. A., Delbridge, E., Purcell, K., Shulkes, A., Kriketos, A., & Proietto, J. (2011). Long-term persistence of hormonal adaptations to weight loss. New England Journal of Medicine, 365(17), 1597–1604. https://doi.org/10.1056/NEJMoa1105816
Supports: appetite hormones (lower leptin, higher ghrelin, higher hunger ratings) persist at least 12 months after diet-induced weight loss and predict regain
Nedeltcheva, A. V., Kilkus, J. M., Imperial, J., Schoeller, D. A., & Penev, P. D. (2010). Insufficient sleep undermines dietary efforts to reduce adiposity. Annals of Internal Medicine, 153(7), 435–441. https://doi.org/10.7326/0003-4819-153-7-201010050-00006
Supports: at identical caloric deficits, shorter sleepers lose 55% less fat and 60% more lean mass than longer sleepers
Tasali, E., Wroblewski, K., Kahn, E., Kilkus, J., & Schoeller, D. A. (2022). Effect of sleep extension on objectively assessed energy intake among adults with overweight in real-life settings: A randomized clinical trial. JAMA Internal Medicine, 182(4), 365–374. https://doi.org/10.1001/jamainternmed.2021.8098
Supports: increasing sleep duration in habitually short sleepers reduces spontaneous energy intake by ~270 kcal/day without conscious diet intervention
Jackson, S. E., Kirschbaum, C., & Steptoe, A. (2017). Hair cortisol and adiposity in a population-based sample of 2,527 men and women aged 54 to 87 years. Obesity, 25(3), 539–544. https://doi.org/10.1002/oby.21733
Supports: persistently elevated long-term cortisol exposure is associated with higher BMI and waist circumference
Balban, M. Y., Neri, E., Kogon, M. M., Weed, L., Nouriani, B., Jo, B., ... & Huberman, A. D. (2023). Brief structured respiration practices enhance mood and reduce physiological arousal. Cell Reports Medicine, 4(1), 100895. https://doi.org/10.1016/j.xcrm.2022.100895
Supports: cyclic sighing produces larger reductions in physiological arousal and improvements in mood than mindfulness in the same time window
Wing, R. R., & Phelan, S. (2005). Long-term weight loss maintenance. American Journal of Clinical Nutrition, 82(1 Suppl), 222S–225S. https://doi.org/10.1093/ajcn/82.1.222S
Supports: National Weight Control Registry maintainers share structural habits including regular self-weighing, consistent eating patterns, daily activity, and high breakfast frequency
Hall, K. D., Heymsfield, S. B., Kemnitz, J. W., Klein, S., Schoeller, D. A., & Speakman, J. R. (2012). Energy balance and its components: Implications for body weight regulation. American Journal of Clinical Nutrition, 95(4), 989–994. https://doi.org/10.3945/ajcn.112.036350
Supports: dynamic interaction of intake, expenditure, and adaptation in body weight regulation
Frequently Asked Questions
Why can't I lose weight even when I'm dieting carefully?
The most common drivers are estimation drift, metabolic adaptation, recovery deficits in sleep and stress, and water masking. The diagnostic step is one week of weighed food intake with daily weigh-ins averaged across the week. Most stalls resolve at the audit step before any biological cause needs consideration.
Why am I not losing weight in a calorie deficit?
Usually because the deficit is smaller in practice than on paper. Adults with diet resistance under-report intake by ~47% and over-report activity by ~50% versus doubly-labeled water measurement. Weighing food in grams for 1-2 weeks resolves most cases. If precision-tracked intake still produces no loss after 3 weeks, metabolic adaptation is the next likely cause and a 1-2 week diet break at maintenance typically restores progress.
What does a real weight loss plateau look like, and what should I do?
Three or more consecutive weeks with no movement in the weekly weight average at a logged deficit. The order of operations is: audit intake by weighing in grams for one week, audit activity, take a 1-2 week diet break at maintenance, and only then reduce calories or increase activity by ~10-15%.
How do I break a weight loss plateau without starving?
The strongest 2026-supported intervention is a structured 1-2 week diet break at maintenance with protein held constant. The MATADOR trial showed intermittent restriction with two-week maintenance breaks produced more total fat loss and less metabolic adaptation than continuous restriction.
How does the sleep and weight loss connection affect a deficit?
Strongly. A randomized trial of adults on identical calorie-restricted diets found that the group sleeping 5.5 hours lost 55% less fat and 60% more lean mass than the group sleeping 8.5 hours over two weeks. A separate trial showed that increasing sleep duration in habitually short sleepers reduced spontaneous intake by ~270 kcal/day without diet intervention.
How do I lose weight sustainably without regaining it?
Target 0.5-1.0% of body weight per week, 15-25% deficit, 0.7-1.0 g/lb protein, 2-3 weekly resistance sessions, stable sleep, planned diet breaks every 6-10 weeks, and a pre-defined maintenance plan. Most regain occurs in the first six months after loss; a structured transition predicts maintenance better than any specific diet pattern.
What habits matter most for long-term weight loss success?
The National Weight Control Registry points to structural habits: regular self-weighing with weekly averaging, protein at every meal, daily step targets that protect NEAT, stable sleep timing, an early-phase food log, defaults for likely-skipped meals, and a planned higher-calorie meal weekly. Routine architecture matters more than diet brand.


