
Why Do I Get Sick So Often? An Evidence-Based Guide to Low Immunity in Adults
Why Do I Get Sick So Often? An Evidence-Based Guide to Low Immunity in Adults
By the HealthPerk Editorial Team · Last updated: May 2026
Quick Answer
Why do I get sick so often?
For most adults who catch more than 4–6 respiratory infections a year, the cause is not a broken immune system but a chronically stressed one. Five recoverable inputs explain the majority of cases: short or fragmented sleep, sustained psychological stress, low-grade nutritional deficiencies (especially vitamin D, zinc, and protein), poor gut barrier function from low-fiber diets and recurrent antibiotic exposure, and high pathogen-contact environments (young children at home, commuting, open-plan offices). True primary immunodeficiency is rare in adults and presents with a specific clinical pattern rather than ordinary frequent colds.
Match the pattern to the most likely driver:
| If the pattern feels like… | Most likely driver | First step |
|---|---|---|
| Every cold turns into a 2–3 week illness | Recovery deficit — sleep and stress | Fix wake time; protect 7–8 hours sleep for 4 weeks |
| Sick within 1–2 weeks of every work crunch | Cortisol-driven immune suppression | Audit chronic stress load; cyclic sighing daily |
| Constant low-grade sniffles, sinus, GI complaints | Mucosal barrier and microbiome | Add 25–30 g/day fiber, fermented foods, screen vitamin D |
| Fatigue, hair loss, slow wound healing alongside infections | Nutritional deficiency | Blood panel: ferritin, vitamin D, B12, zinc |
| Healthy adult, 4–6 colds a year, kids at home | Pathogen exposure, not immune failure | Reasonable expectation; focus on severity, not count |
The experience of catching one infection after another, watching coworkers and family members shrug off the same bug in days while it lingers for weeks, is one of the most common reasons adults search for answers about their immune system. Why do I get sick so often is rarely a question with a single biological cause — it is the convergence of recovery debt, nutritional gaps, environmental exposure, and behavioral patterns that together determine how often the immune system is overwhelmed.
By 2026, the consensus across immunology, sleep medicine, and nutritional science has converged on a more practical view than the older "boost your immunity" framing. The immune system is not a dial that can be turned up; it is a layered defense (physical barriers, innate immunity, adaptive immunity, mucosal IgA, microbiome) whose function depends on the same recovery inputs that govern energy, mood, and metabolic health. The honest answer to "why am I sick again" almost always lies in one of those inputs.
This guide maps the most common drivers of frequent illness in adults using the strongest 2026 evidence, organized by leverage rather than by novelty.
Table of Contents
- Weak Immune System Symptoms
- Signs of Low Immunity
- Low Immunity Causes in Adults
- Frequent Colds: Causes and Patterns
- Why Am I Always Catching Colds
- Sleep and Immunity Connection
- Stress and the Immune System
- Gut Health and the Immune System
- Vitamin Deficiency and Immunity
- Lifestyle Factors Affecting Immunity
- Frequently Asked Questions
- References
Weak Immune System Symptoms

Weak immune system symptoms are pattern-based rather than single-event-based. A single bad cold says nothing. What matters is the frequency, severity, recovery time, and clustering of infections across 6–12 months. Among adults, the symptom profile that signals genuinely under-functioning immune defense includes recurrent upper-respiratory infections (more than 4–6 a year for non-parents), repeated sinus or ear infections in adulthood, recurrent oral or genital herpes outbreaks, slow wound healing, persistent fatigue alongside infections, and frequent low-grade GI complaints.
A useful frame from clinical immunology: severity and chronicity matter more than count. Four ordinary colds a winter in an adult with young kids at home is normal pathogen exposure, not failure. One infection a year that takes 4 weeks to clear, or that descends into bronchitis each time, is a signal.
Getting sick easily immune system patterns
The pattern most associated with getting sick easily immune system dysfunction in adults is repeated infections of the same anatomical area — sinuses, ears, lungs, urinary tract, or skin — within a 12-month window, often combined with disproportionate severity (high fever, lower-respiratory involvement, prolonged recovery). This pattern, especially when it appears in adulthood after years of normal infection frequency, warrants a clinical workup rather than supplement experimentation. Common-variable immunodeficiency, IgA deficiency, and complement deficiencies can present this way and respond to specific medical management.
By contrast, the pattern of "catching every cold that goes around but recovering normally" is almost always a question of exposure and recovery inputs (sleep, stress, nutrition), not of immune competence. Distinguishing the two patterns is the first step in deciding whether to fix lifestyle inputs or seek a primary-care immunology workup.
Signs of Low Immunity
Signs of low immunity worth tracking, in adults who suspect their immune defense is under-performing:
- Frequency — more than 4–6 colds a year in an adult without young children at home
- Severity — colds that descend into bronchitis, sinusitis, or ear infection more than once a year
- Duration — symptoms persisting beyond 14 days when the typical adult cold resolves in 7–10
- Recovery time — post-illness fatigue lasting weeks
- Anatomical recurrence — repeat infections of the same site (sinus, ear, UTI, skin)
- Opportunistic infections — recurrent oral thrush, shingles in adults under 50, persistent warts
- Slow wound healing — minor cuts that take more than 7–10 days to close
- Recurrent mouth ulcers — beyond once or twice a year
- Chronic GI symptoms alongside infections — suggesting mucosal-immune compromise
Poor immune system symptoms that warrant medical workup
Poor immune system symptoms that should prompt evaluation by a primary care physician or immunologist include: two or more pneumonias in one year, two or more severe sinus infections, two or more months of oral antibiotics with little effect, recurrent deep skin or organ abscesses, persistent thrush after age 1, need for IV antibiotics to clear infections, two or more invasive infections (meningitis, osteomyelitis, cellulitis, sepsis), or a family history of primary immunodeficiency. The Jeffrey Modell Foundation's "10 warning signs" of primary immunodeficiency, endorsed in the AAAAI practice parameter (Bonilla et al., 2015), organize this evaluation; any two warrant an immunology referral.
A baseline blood panel for adults with this pattern typically includes CBC with differential, immunoglobulin levels (IgG, IgA, IgM), HIV testing where appropriate, vitamin D, ferritin, and zinc — the combination distinguishes treatable nutritional or hormonal contributors from less-common primary immune disorders.
Low Immunity Causes in Adults
Low immunity causes adults experience are usually behavioral and environmental rather than congenital. The biggest contributors, ranked by typical effect size:
- Sleep deprivation and irregularity. The clearest single lever, with multiple randomized trials documenting reduced antibody response to vaccines and increased respiratory-infection rates after short sleep (Prather et al., 2015; Spiegel et al., 2002).
- Chronic psychological stress. Sustained cortisol exposure suppresses lymphocyte function and shifts the immune balance toward inflammation. A meta-analysis of 293 studies confirmed reduced immune competence with chronic stress exposure (Segerstrom & Miller, 2004).
- Micronutrient deficiencies. Vitamin D below 20 ng/mL, low zinc, low selenium, and inadequate protein intake all measurably reduce immune function. Vitamin D deficiency is particularly common in 2026 in adults working indoors at northern latitudes.
- Gut microbiome disruption. Low-fiber diets, recurrent antibiotic exposure, and ultra-processed-food patterns reduce microbial diversity, which in turn weakens the gut-associated immune tissue (GALT) where the largest share of immune cells resides.
- Sedentary behavior and lack of moderate exercise. A J-curve effect: regular moderate exercise enhances immune surveillance; prolonged sedentary patterns and over-training both depress it.
- Smoking, vaping, and heavy alcohol use. All damage mucosal barriers and impair phagocyte function.
- Aging and undiagnosed chronic disease. Type 2 diabetes, hypothyroidism, and chronic kidney disease all reduce immune competence; immune function declines gradually after age 60 (immunosenescence).
- Medications. Systemic corticosteroids, biologics, chemotherapy, and even chronic NSAID use can blunt immune function.
- Stress on the mucosal barrier. Dry indoor air, dehydration, mouth-breathing during sleep, and chronic sinus inflammation reduce the physical first line of defense.
The practical implication: most adults with frequent infections do not have a broken immune system. They have multiple sub-clinical inputs running below optimal, and the fix is leverage-stacked across the top 3–4 inputs rather than any single magic intervention.
Frequent Colds: Causes and Patterns
Frequent colds causes in adults fall into two broad categories: exposure-driven and host-driven. The distinction matters because the fix is different for each.
Exposure-driven frequent colds are the more common pattern. Adults with young children at home are exposed to 8–12 distinct respiratory viruses per cold season as children import infections from school and daycare; this drives a normal increase in adult infection count that has nothing to do with immune competence. Healthcare workers, teachers, retail and hospitality staff, and adults who commute on crowded public transit have similarly elevated exposure baselines. The corrective is not "boost immunity" but realistic expectations and exposure hygiene — hand washing on entry home, not touching the face between exposure and washing, and humidified indoor air in winter to keep nasal mucus barrier intact.
Host-driven frequent colds reflect the recovery deficits described above. The clearest behavioral marker is whether each cold is unusually severe or prolonged, not just whether the count is high. A 2015 Sleep trial inoculated 164 healthy adults with rhinovirus after monitoring sleep for one week; those sleeping fewer than 6 hours were 4.2× more likely to develop a clinical cold than those sleeping more than 7 hours (Prather et al., 2015). The same exposure produced different outcomes based on host recovery state.
A useful diagnostic question: "Of the last five colds I caught, did I catch them from an obvious source, or did they appear without traceable exposure?" If almost every cold has a clear source (sick child, sick coworker), exposure is the dominant driver and the lever is mucosal-barrier care and realistic expectations. If colds appear without traceable source and recovery is slow, host factors dominate and the lever is sleep, stress, and nutrition.
Why Am I Always Catching Colds
Why am I always catching colds is among the most-searched immune-system questions, and the honest answer combines exposure and host factors in a way most "boost your immunity" content sidesteps.
The 2026 evidence-supported interventions that meaningfully reduce respiratory infection rate, ranked by effect size:
- Consistent sleep duration ≥7 hours. The single highest-yield lever, per Prather et al. (2015) and replicated in observational cohorts.
- Hand hygiene at transition points. A 2020 Cochrane review of 67 trials found regular handwashing reduced respiratory infection transmission by ~16–21% across community settings (Jefferson et al., 2020). The effect compounds when combined with not touching the face.
- Vaccination per current guidance. Annual influenza, periodic SARS-CoV-2 boosters per regional guidance, and pneumococcal vaccination as indicated remain among the largest single-effect interventions.
- Vitamin D sufficiency. A 2017 BMJ meta-analysis of 25 trials (11,321 participants) found vitamin D supplementation reduced acute respiratory infection rates, with the largest effect in the deficient (Martineau et al., 2017).
- Indoor humidity 40–60%. Dry indoor air dehydrates nasal mucus, impairing mucociliary clearance.
- Mask use during community waves of respiratory illness. Modest but real effect in high-exposure periods.
- Moderate exercise 150–300 min/week. Supports immune surveillance without the suppression seen at very high training volumes.
What does not meaningfully change adult infection rate, per current evidence: high-dose vitamin C for prevention, generic "immune-boosting" multivitamins in already-replete adults, echinacea or elderberry as primary prevention (modest at best), and saline-only nasal sprays without other interventions.
If the count exceeds 6–8 distinct infections a year in an adult without young children at home, or if individual infections are unusually severe or prolonged, the appropriate next step is a primary care evaluation rather than additional supplements.
Sleep and Immunity Connection
The sleep and immunity connection is one of the most robustly documented relationships in immunology. Multiple lines of evidence converge: sleep deprivation reduces antibody response to vaccines, increases circulating inflammatory cytokines while reducing protective immune responses, raises susceptibility to experimental viral inoculation, and impairs the nighttime consolidation processes that move antigens through the immune system.
A 2002 JAMA trial sleep-restricted healthy young men to 4 hours nightly across 6 nights, vaccinating them against influenza on day 4 of restriction; antibody titers were less than half those of well-rested controls measured 10 days post-vaccination (Spiegel et al., 2002). A 2015 Sleep trial cited above documented a 4.2× increase in clinical cold incidence after rhinovirus exposure in adults sleeping under 6 hours per night (Prather et al., 2015). A 2019 Journal of Experimental Medicine paper described the mechanism: sleep enhances T-cell adhesion to antigen-presenting cells through reduced sympathetic-adrenergic signaling, improving immune-memory formation (Dimitrov et al., 2019).
Mechanisms with the strongest 2026 evidence:
- Deep sleep windows host the largest spikes in growth hormone and prolactin, both of which support T-cell proliferation
- Sympathetic nervous system activity drops in deep sleep, freeing T-cells to bind antigen-presenting cells more efficiently
- Sleep loss elevates IL-6, TNF-α, and other inflammatory cytokines, biasing immune output toward inflammation rather than targeted defense
- Circadian disruption alone (without total sleep loss) measurably reduces NK-cell activity
Practical levers, in order of effect:
- Fix wake time first. A 30-minute weekend window; regularity outranks duration alone.
- Protect 7–8 hours of opportunity. Short sleep is the input the immune system tolerates worst.
- Cool, dark bedroom (16–19 °C), screens out in the last 60 minutes.
- 10 minutes of outdoor daylight within 30 minutes of waking. Anchors circadian phase, supports natural melatonin rhythm.
- Cap caffeine at 14:00 if metabolism is slow; later caffeine fragments slow-wave sleep without subjective awareness.
- Screen for sleep apnea if snoring, witnessed pauses, or unrefreshing sleep are present; untreated apnea is independently associated with reduced immune competence.
Of all the non-vaccination immune interventions, sleep regularity has the best ratio of effect size to required effort.
Stress and the Immune System
Stress and immune system function are linked through measurable hormonal, cellular, and behavioral pathways. The short version of decades of research: brief, acute stress can transiently mobilize immune defenses; sustained, chronic stress reliably suppresses them.
A 2004 Psychological Bulletin meta-analysis of 293 studies by Segerstrom and Miller found that brief stressors (a few minutes to an hour) tended to enhance natural-immunity measures, while chronic stressors (months to years — job strain, caregiving, unemployment, bereavement) systematically reduced both cellular and humoral immunity, with effect sizes increasing with duration of the stressor (Segerstrom & Miller, 2004). The implication is not "avoid all stress" — short stressors are mostly fine — but that sustained stress without recovery windows is the immune-relevant pattern.
Mechanisms with the strongest evidence:
- Chronic cortisol elevation suppresses lymphocyte proliferation and shifts cytokine balance toward Th2 patterns less effective at clearing viral infections
- Sympathetic activation reduces NK-cell trafficking and antibody response over time
- Stress disrupts sleep, which compounds immune suppression independently
- Stress shifts behavior — less exercise, more ultra-processed food, more alcohol — that further reduces immune competence
Recovery interventions with the strongest 2026 evidence:
- Cyclic sighing — 2 nasal inhales, slow mouth exhale, repeated for 5 minutes daily. A 2023 Cell Reports Medicine trial by Balban and colleagues found cyclic sighing reduced physiological arousal and improved mood more than mindfulness meditation in the same time window (Balban et al., 2023).
- Outdoor walking, 20+ minutes daily. Reliably reduces cortisol and supports adherence to other immune-relevant habits.
- Maintained social contact. Loneliness is independently associated with elevated inflammation; brief regular in-person connection reduces next-day cortisol.
- Restored sleep, as above — stress and sleep are coupled and improve together.
The immune payoff is rarely immediate; effects on infection rate compound over weeks, not days.
Gut Health and the Immune System
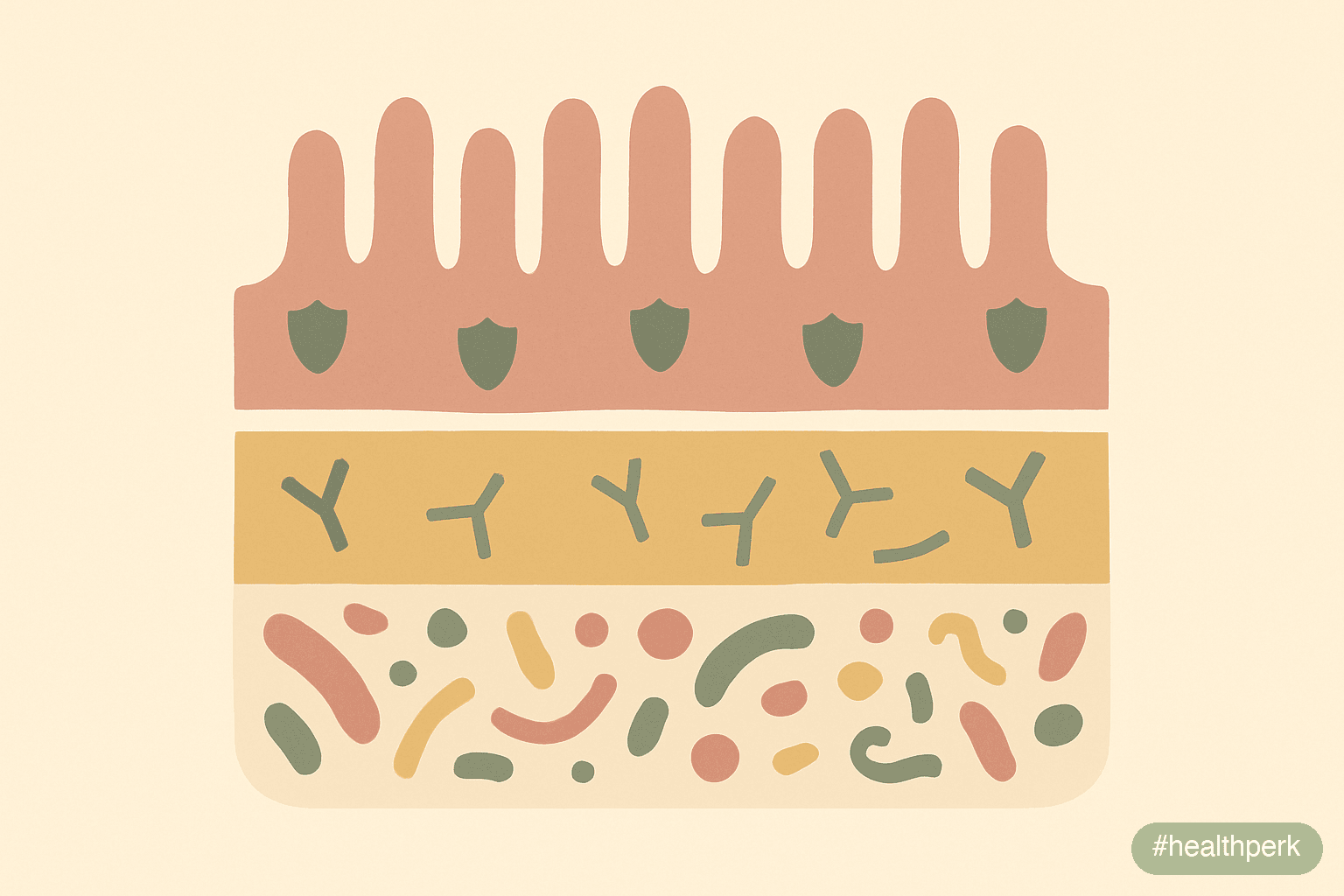
Gut health and immune system function are inseparable: roughly 70–80% of the body's immune cells reside in or are influenced by gut-associated lymphoid tissue (GALT), and the gut microbiome is one of the largest single inputs to immune calibration. A 2026 adult eating a low-fiber Western diet typically harbors lower microbial diversity than ancestral or non-industrial comparison populations, with measurable downstream effects on inflammatory tone and mucosal immunity.
The strongest evidence-based levers for gut-immune function:
- Dietary fiber, 25–35 g/day from diverse plant sources. Short-chain fatty acids produced by fiber fermentation (especially butyrate) support gut barrier integrity, regulatory T-cell development, and IgA production. A 2021 Cell trial showed a 10-week high-fermented-food diet measurably reduced inflammatory markers in adults with adequate baseline microbiome diversity (Wastyk et al., 2021).
- Fermented foods 1–3 servings daily. The same Stanford 10-week trial found that fermented food intake increased microbiome diversity and decreased 19 inflammatory proteins, an effect not seen with fiber alone — suggesting complementary mechanisms.
- Targeted probiotic strains for specific contexts. L. rhamnosus GG and B. lactis have the strongest trial evidence for reducing respiratory and GI infection rates, especially in children and the elderly (King et al., 2014).
- Avoiding unnecessary antibiotics. Each course measurably reduces microbial diversity, with partial recovery taking weeks to months; cumulative lifetime exposure correlates with adult immune outcomes.
- Polyphenol-rich foods. Berries, tea, coffee, olive oil, and dark chocolate supply substrates that beneficial microbes preferentially metabolize.
- Sleep regularity. Circadian rhythms entrain gut microbial composition; chronic sleep disruption shifts the microbiome toward inflammatory profiles.
What does not work: indiscriminate "high-CFU" probiotic supplements without strain specificity, gut "cleanses," elimination diets without diagnosed sensitivity, or replacing whole-food fiber with isolated fiber powders. The microbiome responds to the totality of the dietary pattern, not to single ingredients.
Vitamin Deficiency and Immunity
Vitamin deficiency and immunity are linked at multiple levels: vitamins serve as cofactors for immune-cell metabolism, antibody synthesis, and pathogen clearance. The 2026 evidence is clearest for a small set of micronutrients where adult deficiency is common in industrialized settings and where repletion measurably improves immune outcomes.
- Vitamin D. The single best-studied immune-relevant micronutrient. The 2017 BMJ meta-analysis of 25 RCTs (11,321 participants) by Martineau and colleagues found vitamin D supplementation reduced acute respiratory infections, with the strongest effect (adjusted OR ~0.30) in those with baseline serum 25(OH)D below 25 nmol/L (Martineau et al., 2017). Replete first; do not over-supplement. Most adults in northern latitudes during winter benefit from 1,000–2,000 IU/day with a target serum level of 30–50 ng/mL.
- Zinc. A cofactor for over 300 enzymes including those in immune-cell function. Deficiency is more common than commonly assumed in older adults and vegetarian patterns. Short-course zinc lozenges (75 mg/day elemental, started within 24 hours of cold onset) have moderate trial evidence for shortening cold duration (Hemilä, 2017); chronic high-dose use is not warranted because it impairs copper absorption.
- Vitamin C. Routine high-dose supplementation does not prevent colds in the general population but may modestly shorten duration. The exception is high physical-stress contexts (marathoners, soldiers, mountaineers) where prevention effects appear (Hemilä & Chalker, 2013).
- Vitamin A. Critical for mucosal barrier and IgA production; deficiency is rare in adults eating any animal foods or orange/dark-green vegetables.
- Iron. Both deficiency and excess impair immunity. Test before supplementing.
- Protein. Often overlooked. Inadequate protein (under ~0.6 g/lb body weight) measurably reduces antibody production and immune-cell turnover. Adults in calorie-restricted or eating-disordered patterns are at risk.
- Selenium. Deficiency reduces antibody response and antioxidant capacity; one Brazil nut a day covers requirements for most adults.
The practical implication: rather than empirically taking a "multivitamin for immunity," ask a primary care provider for a basic panel — vitamin D, ferritin, B12, and zinc — and replete what is documented low. Repletion is reliably effective; supplementation in already-replete adults rarely is.
Lifestyle Factors Affecting Immunity
Lifestyle factors affecting immunity are the structural choices that determine whether immune function operates at the high end or the low end of an adult's individual range. None of the levers below are novel; their cumulative effect is what matters.
The factors with the strongest 2026 evidence for reducing infection rate, severity, and duration:
- Stable sleep timing and duration ≥7 hours. Largest single non-vaccination lever.
- Moderate exercise, 150–300 min/week. A J-curve effect — both sedentary patterns and high-volume training above 600 min/week of intense work increase infection risk. The middle range reliably supports immune surveillance (Nieman & Wentz, 2019).
- Adequate protein, 0.6–0.8 g/lb body weight, distributed across meals. Supports antibody and immune-cell synthesis.
- 25–35 g fiber daily from diverse plant sources. Supports microbiome diversity and short-chain fatty acid production.
- Limited alcohol — under 5 drinks/week, no binges. Heavy drinking measurably impairs phagocyte function and mucosal barrier.
- No smoking, no vaping. Both damage cilia and mucosal immunity.
- Indoor humidity 40–60% during heating season. Protects nasal mucus barrier.
- Hand hygiene at transition points — entering home, before eating, after using shared surfaces.
- Up-to-date vaccinations per current regional guidance.
- Body weight in a healthy range. Obesity is associated with chronic low-grade inflammation and reduced response to several vaccines; weight loss reverses much of the effect.
- Limiting ultra-processed food. Independent associations with inflammatory tone after controlling for calories.
- Daylight exposure, 10+ minutes within 30 minutes of waking. Supports circadian-immune coupling.
A useful frame: immune function is a downstream readout of the basic recovery and metabolic state of the body. Most "boost your immunity" marketing aims at single ingredients; the evidence supports stacking 4–5 of the above levers and maintaining them across seasons. People who rarely catch infections in the same exposure environment as those who catch frequent ones almost always differ on multiple of these structural inputs.
Related Articles on HealthPerk
Explore more on this topic:
- How to Boost the Immune System Naturally
- Best Vitamins and Supplements for Immunity
- Foods That Boost the Immune System
- How to Stop Overthinking
- How to Lose Weight Sustainably
Frequently Asked Questions
Why do I get sick so often as a healthy adult?
For most healthy adults, frequent infections reflect a combination of normal exposure (especially with young children at home or in crowded work settings) and recovery deficits that lower defense — short sleep, sustained psychological stress, low-grade nutritional gaps (vitamin D, zinc, protein), and gut microbiome disruption. True primary immunodeficiency is rare and presents with a specific pattern: repeated severe infections of the same anatomical site, infections requiring IV antibiotics, recurrent oral thrush, or unusual opportunistic infections. The diagnostic step is to evaluate whether infections are unusually severe or prolonged (host factor) or simply frequent in a high-exposure environment (exposure factor) — the corrective is different for each.
What are weak immune system symptoms in adults?
Pattern-based rather than single-event-based: more than 4–6 colds per year in an adult without young children at home, infections that descend into bronchitis or sinusitis, individual infections lasting beyond 14 days, recurrent infections of the same anatomical area (sinus, ear, urinary tract, skin), slow wound healing, recurrent oral or genital herpes outbreaks, recurrent mouth ulcers, persistent fatigue alongside infections, and chronic low-grade GI symptoms. Two or more of these warrant a primary-care visit and a basic blood panel including CBC with differential, immunoglobulin levels, vitamin D, ferritin, and zinc.
What does getting sick easily say about your immune system?
Getting sick easily — meaning catching infections from minimal exposure — is more often a host-state signal (sleep debt, stress, nutritional gaps) than a sign of structural immune defect. A 2015 trial inoculated 164 adults with rhinovirus after monitoring sleep: those sleeping under 6 hours were 4.2 times more likely to develop a clinical cold than those sleeping over 7. Same virus, same dose, different host state. Repeated infections of the same anatomical site or unusually severe infections are different patterns and warrant clinical evaluation rather than lifestyle adjustment alone.
What are the main low immunity causes in adults?
Ranked by typical effect size: sleep deprivation and irregularity, chronic psychological stress, micronutrient deficiencies (especially vitamin D, zinc, and protein), gut microbiome disruption from low-fiber diets and recurrent antibiotics, sedentary patterns or over-training, smoking or heavy alcohol use, undiagnosed chronic disease (type 2 diabetes, hypothyroidism, kidney disease), specific medications (corticosteroids, biologics, chemotherapy), and aging (immunosenescence after 60). Most adults with frequent infections have several of these inputs running below optimal rather than a single failure; the fix is leverage-stacked across the top 3–4 inputs.
Why am I always catching colds when others around me are not?
The two most likely explanations are different exposure (an adult with kids in daycare catches more viruses than a single adult working from home, with nothing wrong on either side) and different host state (a sleep-restricted, stressed adult is 4× more susceptible to the same viral dose than a rested adult). Audit both: how many distinct exposures per week, and what is your sleep, stress, and nutritional baseline? If colds are not just frequent but unusually severe or prolonged, the host-state explanation dominates and the levers are sleep, stress, vitamin D, and gut health rather than additional supplements.
How are frequent colds causes linked to sleep?
A 2015 Sleep trial inoculated 164 adults with rhinovirus and monitored sleep for one week; those sleeping under 6 hours were 4.2 times more likely to develop a clinical cold than those sleeping over 7. A 2002 JAMA trial showed sleep-restricted adults developed less than half the antibody titers of rested controls after influenza vaccination. Sleep enhances T-cell adhesion to antigen-presenting cells in deep-sleep windows, with measurable effects on immune-memory formation. Of all the non-vaccination immune levers, sleep regularity has the best ratio of effect size to required effort.
How does the sleep and immunity connection work mechanically?
Deep sleep windows host peaks in growth hormone and prolactin that support T-cell proliferation; sympathetic nervous system activity drops, freeing T-cells to bind antigen-presenting cells more efficiently; sleep loss elevates IL-6 and TNF-α, biasing immune output toward inflammation rather than targeted defense; and circadian disruption alone (independent of total sleep loss) reduces natural-killer-cell activity. The practical implication is that fixing wake-time regularity and protecting 7–8 hours of sleep opportunity is among the highest-yield immune interventions available.
How do stress and the immune system interact in practice?
Brief acute stress (minutes to an hour) tends to enhance natural-immunity measures, while chronic stress (months to years — job strain, caregiving, unemployment, bereavement) systematically reduces both cellular and humoral immunity, with effects increasing with duration. Mechanisms include chronic cortisol suppression of lymphocyte proliferation, sympathetic activation reducing natural-killer cell trafficking, and stress-driven disruption of sleep and behavior. The corrective levers are daily cyclic sighing, outdoor walking, maintained social contact, and restored sleep — all of which compound over weeks rather than days.
How does gut health and immune system function connect?
About 70–80% of immune cells reside in or are influenced by gut-associated lymphoid tissue. Dietary fiber feeds microbes that produce short-chain fatty acids (especially butyrate), which support gut barrier integrity and regulatory T-cell development. A 10-week Stanford trial found that combining 25–35 g daily fiber with 1–3 daily servings of fermented foods increased microbiome diversity and decreased 19 inflammatory proteins. Avoiding unnecessary antibiotics, eating polyphenol-rich foods, and maintaining sleep regularity are the dominant levers; indiscriminate probiotic supplementation without strain specificity has weaker evidence.
What vitamin deficiency and immunity links matter most?
Vitamin D is the best-studied, with a 2017 meta-analysis of 25 RCTs showing supplementation reduces acute respiratory infections — strongest effect in the deficient. Zinc deficiency impairs immune-cell function; short-course lozenges (75 mg/day, within 24 hours of cold onset) modestly shorten duration. Adequate protein (0.6–0.8 g/lb body weight) is often overlooked but essential for antibody synthesis. Iron deficiency impairs immunity; excess does too — test before supplementing. The best approach is a basic blood panel (vitamin D, ferritin, B12, zinc) and repletion of documented deficiencies rather than empirical multivitamin use in already-replete adults.
What lifestyle factors affecting immunity should I prioritize first?
In order of effect: stable sleep timing with 7–8 hours of opportunity, moderate exercise 150–300 minutes per week (avoiding both sedentary and excessive patterns), adequate protein and 25–35 g daily fiber, limiting alcohol to under 5 drinks per week with no binges, no smoking or vaping, indoor humidity 40–60% during heating season, hand hygiene at transition points, up-to-date vaccinations, body weight in a healthy range, limiting ultra-processed food, and daylight exposure within 30 minutes of waking. The cumulative effect of stacking 4–5 of these levers reliably outperforms any single "immune-boosting" supplement.
This article is for informational purposes only and does not constitute medical advice. Frequent or severe infections may signal treatable conditions including primary or secondary immunodeficiency, HIV, undiagnosed diabetes, hypothyroidism, chronic kidney disease, malnutrition, and side effects of common medications. Consult a qualified healthcare provider if you experience two or more pneumonias in a year, repeated severe sinus infections, infections requiring intravenous antibiotics, recurrent oral thrush after age 1, unusual opportunistic infections, or a family history of primary immunodeficiency. Do not start or stop prescription medications without supervision. Individual results may vary.
About the author The HealthPerk Editorial Team reviews immune-system research through evidence synthesis cross-referenced with peer-reviewed clinical trials and clinical practice guidelines. Our immunity content is reviewed for medical accuracy against current immunology, infectious-disease, and clinical-immunology standards. How we review →
References
Bonilla, F. A., Khan, D. A., Ballas, Z. K., Chinen, J., Frank, M. M., Hsu, J. T., ... & Wallace, D. (2015). Practice parameter for the diagnosis and management of primary immunodeficiency. Journal of Allergy and Clinical Immunology, 136(5), 1186–1205. https://doi.org/10.1016/j.jaci.2015.04.049
Supports: clinical warning signs of primary immunodeficiency in adults, including pneumonia frequency, recurrent sinus infections, IV-antibiotic-dependence, recurrent thrush, and invasive infections
Prather, A. A., Janicki-Deverts, D., Hall, M. H., & Cohen, S. (2015). Behaviorally assessed sleep and susceptibility to the common cold. Sleep, 38(9), 1353–1359. https://doi.org/10.5665/sleep.4968
Supports: adults sleeping under 6 hours were 4.2× more likely to develop a clinical cold after experimental rhinovirus exposure compared with those sleeping over 7 hours
Spiegel, K., Sheridan, J. F., & Van Cauter, E. (2002). Effect of sleep deprivation on response to immunization. JAMA, 288(12), 1471–1472. https://doi.org/10.1001/jama.288.12.1471-a
Supports: sleep-restricted adults developed less than half the antibody titers of rested controls 10 days after influenza vaccination
Segerstrom, S. C., & Miller, G. E. (2004). Psychological stress and the human immune system: A meta-analytic study of 30 years of inquiry. Psychological Bulletin, 130(4), 601–630. https://doi.org/10.1037/0033-2909.130.4.601
Supports: chronic stress (months to years) systematically reduces cellular and humoral immunity, with effect sizes increasing with stressor duration
Martineau, A. R., Jolliffe, D. A., Hooper, R. L., Greenberg, L., Aloia, J. F., Bergman, P., ... & Camargo, C. A. (2017). Vitamin D supplementation to prevent acute respiratory tract infections: Systematic review and meta-analysis of individual participant data. BMJ, 356, i6583. https://doi.org/10.1136/bmj.i6583
Supports: vitamin D supplementation reduces acute respiratory infection incidence, with strongest effect in baseline-deficient adults
Jefferson, T., Del Mar, C. B., Dooley, L., Ferroni, E., Al-Ansary, L. A., Bawazeer, G. A., ... & Conly, J. M. (2020). Physical interventions to interrupt or reduce the spread of respiratory viruses. Cochrane Database of Systematic Reviews, (11). https://doi.org/10.1002/14651858.CD006207.pub5
Supports: regular handwashing reduces respiratory infection transmission by ~16–21% across community settings
Dimitrov, S., Lange, T., Gouttefangeas, C., Jensen, A. T. R., Szczepanski, M., Lehnnolz, J., ... & Born, J. (2019). Gαs-coupled receptor signaling and sleep regulate integrin activation of human antigen-specific T cells. Journal of Experimental Medicine, 216(3), 517–526. https://doi.org/10.1084/jem.20181169
Supports: sleep enhances T-cell adhesion to antigen-presenting cells through reduced sympathetic-adrenergic signaling, improving immune-memory formation
Wastyk, H. C., Fragiadakis, G. K., Perelman, D., Dahan, D., Merrill, B. D., Yu, F. B., ... & Sonnenburg, J. L. (2021). Gut-microbiota-targeted diets modulate human immune status. Cell, 184(16), 4137–4153. https://doi.org/10.1016/j.cell.2021.06.019
Supports: a 10-week dietary intervention combining fiber and fermented foods increased microbiome diversity and reduced 19 inflammatory proteins in healthy adults
Hemilä, H. (2017). Zinc lozenges and the common cold: A meta-analysis comparing zinc acetate and zinc gluconate, and the role of zinc dosage. JRSM Open, 8(5), 2054270417694291. https://doi.org/10.1177/2054270417694291
Supports: zinc lozenges at 75 mg/day started within 24 hours of symptom onset modestly shorten common-cold duration
Nieman, D. C., & Wentz, L. M. (2019). The compelling link between physical activity and the body's defense system. Journal of Sport and Health Science, 8(3), 201–217. https://doi.org/10.1016/j.jshs.2018.09.009
Supports: a J-curve relationship between exercise volume and immune competence — moderate activity supports immune surveillance while sedentary and very high-volume training both increase infection risk
- Balban, M. Y., Neri, E., Kogon, M. M., Weed, L., Nouriani, B., Jo, B., ... & Huberman, A. D. (2023). Brief structured respiration practices enhance mood and reduce physiological arousal. Cell Reports Medicine, 4(1), 100895. https://doi.org/10.1016/j.xcrm.2022.100895
Supports: cyclic sighing performed 5 minutes daily reduced physiological arousal and improved mood more than mindfulness meditation in a randomized trial
- King, S., Glanville, J., Sanders, M. E., Fitzgerald, A., & Varley, D. (2014). Effectiveness of probiotics on the duration of illness in healthy children and adults who develop common acute respiratory infectious conditions: A systematic review and meta-analysis. British Journal of Nutrition, 112(1), 41–54. https://doi.org/10.1017/S0007114514000075
Supports: targeted probiotic strains including L. rhamnosus GG and B. lactis reduce respiratory and gastrointestinal infection rates, especially in children and older adults
- Hemilä, H., & Chalker, E. (2013). Vitamin C for preventing and treating the common cold. Cochrane Database of Systematic Reviews, (1). https://doi.org/10.1002/14651858.CD000980.pub4
Supports: routine high-dose vitamin C does not prevent colds in the general population but shows preventive effect in high physical-stress contexts such as marathon runners
Frequently Asked Questions
Why do I get sick so often as a healthy adult?
For most healthy adults, frequent infections reflect a combination of normal exposure (especially with young children at home or in crowded work settings) and recovery deficits — short sleep, sustained psychological stress, low-grade nutritional gaps (vitamin D, zinc, protein), and gut microbiome disruption. True primary immunodeficiency is rare and presents with a specific pattern of repeated severe infections of the same anatomical site, infections requiring IV antibiotics, or recurrent thrush.
What are weak immune system symptoms in adults?
Pattern-based markers include more than 4–6 colds per year in adults without young children at home, infections that descend into bronchitis or sinusitis, individual infections lasting beyond 14 days, recurrent infections of the same anatomical area, slow wound healing, recurrent oral or genital herpes outbreaks, recurrent mouth ulcers, and persistent fatigue alongside infections. Two or more warrant a basic blood panel.
What does getting sick easily say about your immune system?
Getting sick easily is more often a host-state signal (sleep debt, stress, nutritional gaps) than a structural immune defect. A 2015 trial showed adults sleeping under 6 hours were 4.2× more likely to develop a clinical cold after the same viral exposure as adults sleeping over 7. Repeated infections of the same anatomical site or unusually severe infections are different patterns and warrant clinical evaluation.
What are the main low immunity causes in adults?
Ranked by typical effect size: sleep deprivation, chronic stress, micronutrient deficiencies (vitamin D, zinc, protein), gut microbiome disruption, sedentary patterns or over-training, smoking or heavy alcohol, undiagnosed chronic disease, specific medications, and aging. Most adults with frequent infections have several inputs below optimal; the fix is leverage-stacked across the top 3–4.
Why am I always catching colds when others around me are not?
The two most likely explanations are different exposure (an adult with kids in daycare catches more viruses than a single adult working from home) and different host state (a sleep-restricted, stressed adult is 4× more susceptible to the same viral dose). Audit both: distinct exposures per week and sleep, stress, and nutritional baseline.
How are frequent colds causes linked to sleep?
A 2015 trial showed adults sleeping under 6 hours were 4.2× more likely to develop a clinical cold than those sleeping over 7. A 2002 JAMA trial showed sleep-restricted adults developed less than half the antibody titers of rested controls after influenza vaccination. Sleep regularity has the best ratio of effect size to effort among non-vaccination immune interventions.
How does the sleep and immunity connection work mechanically?
Deep sleep windows host peaks in growth hormone supporting T-cell proliferation; sympathetic activity drops, freeing T-cells to bind antigen-presenting cells efficiently; sleep loss elevates IL-6 and TNF-α biasing output toward inflammation; and circadian disruption reduces natural-killer-cell activity. Fixing wake-time regularity is among the highest-yield immune interventions.
How do stress and the immune system interact in practice?
Brief acute stress tends to enhance natural-immunity measures; chronic stress systematically reduces cellular and humoral immunity with effects increasing over months and years. Mechanisms include cortisol suppression of lymphocyte proliferation and sympathetic reduction of natural-killer-cell trafficking. Corrective levers are daily cyclic sighing, outdoor walking, social contact, and restored sleep.
How does gut health and immune system function connect?
About 70–80% of immune cells reside in or are influenced by gut-associated lymphoid tissue. Dietary fiber feeds microbes producing short-chain fatty acids that support gut barrier integrity and regulatory T-cell development. A 10-week Stanford trial found fiber plus fermented foods increased microbiome diversity and decreased 19 inflammatory proteins.
What vitamin deficiency and immunity links matter most?
Vitamin D is the best-studied — a 2017 meta-analysis of 25 RCTs showed supplementation reduces acute respiratory infections, strongest effect in the deficient. Zinc deficiency impairs immune-cell function; short-course lozenges (75 mg/day within 24 hours of cold onset) modestly shorten duration. Adequate protein (0.6–0.8 g/lb body weight) is essential for antibody synthesis.
What lifestyle factors affecting immunity should I prioritize first?
Stable sleep with 7–8 hours of opportunity, moderate exercise 150–300 min/week, adequate protein and 25–35 g daily fiber, limiting alcohol, no smoking or vaping, indoor humidity 40–60%, hand hygiene at transitions, up-to-date vaccinations, healthy body weight, limiting ultra-processed food, and daylight within 30 minutes of waking. Stacking 4–5 levers outperforms any single supplement.
More from Supplements


