
Iron Deficiency Fatigue Symptoms: The 2026 Evidence-Based Guide
Iron Deficiency Fatigue Symptoms: The 2026 Evidence-Based Guide
By the HealthPerk Editorial Team · Last updated: May 2026
Quick Answer
How do I know if my fatigue is from iron deficiency?
Iron deficiency fatigue symptoms present as a persistent, exercise-disproportionate tiredness that does not respond to sleep, often paired with one or more recognizable clues: breathlessness on stairs, pallor inside the lower eyelids and palms, brittle or spoon-shaped nails (koilonychia), hair shedding, brain fog, restless legs at night, ice cravings (pagophagia), and a faster resting heart rate. The fatigue has a clear mechanism: iron is essential for hemoglobin synthesis (oxygen delivery), myoglobin (muscle oxygen storage), and the iron-sulfur clusters that power mitochondrial electron transport — so depleted iron simultaneously impairs oxygen transport, muscle function, and cellular energy production (Lopez et al., 2016; Pasricha et al., 2021). Crucially, iron deficiency causes fatigue before anemia develops: ferritin below 30 ng/mL with normal hemoglobin (iron deficiency without anemia) is enough to drive symptoms in many adults, especially menstruating women (Pratt & Khan, 2016). The 2026 default workup asks for ferritin and CBC together — never hemoglobin alone.
Use this triage to decide where to start:
| If your fatigue is paired with… | Likely stage | First test |
|---|---|---|
| Heavy periods, breathlessness on stairs, pallor, ice cravings | Iron deficiency anemia | CBC + ferritin + transferrin saturation |
| Tiredness, hair shedding, restless legs — normal hemoglobin | Iron deficiency without anemia | Ferritin (target >30 ng/mL, ideally >50 ng/mL) |
| Postpartum exhaustion beyond 6 weeks | Postpartum iron depletion | CBC + ferritin |
| Endurance athlete with declining performance | Exercise-induced iron loss | Ferritin + transferrin saturation |
| Vegetarian/vegan with persistent fatigue | Low intake or absorption | Ferritin, CBC, dietary review |
| Older adult, new-onset iron deficiency | Bleeding source workup mandatory | Ferritin + colonoscopy referral |
Iron deficiency is the most common nutritional deficiency in the world and the single most common cause of unexplained fatigue in adults who menstruate (Lopez et al., 2016; Pasricha et al., 2021). Yet it remains under-diagnosed for two reasons: many primary-care visits screen only hemoglobin, which can stay normal for months while body iron stores quietly fall; and ferritin is interpreted against legacy thresholds (>12 or >15 ng/mL) that miss adults who are symptomatic at 20–30 ng/mL. The 2026 picture has moved toward early testing with a higher symptomatic ferritin threshold, alternate-day oral iron dosing, and a broader role for intravenous iron when oral fails. This guide covers exactly what iron deficiency fatigue feels like, how it is confirmed, who is at risk, and which iron supplements for fatigue women actually absorb without wrecking the gut.
Table of Contents
- Iron Deficiency Fatigue Symptoms: How It Actually Feels
- Iron Deficiency Without Anemia: Why Ferritin Matters More Than Hemoglobin
- Who Is at Highest Risk in 2026
- How Iron Deficiency Is Diagnosed: The Right Panel
- Iron Supplements for Fatigue in Women: Dosage, Forms, and What Actually Absorbs
- Food Sources and Absorption Hacks
- When Oral Iron Fails: Intravenous Iron in 2026
- Frequently Asked Questions
- References
Iron Deficiency Fatigue Symptoms: How It Actually Feels
The classic textbook description of iron deficiency leans on overt anemia: pallor, breathlessness on exertion, palpitations, headaches. The clinic picture in 2026 is earlier and broader. Most adults who eventually meet anemia criteria pass through months — sometimes years — of symptomatic iron deficiency with normal or borderline hemoglobin, during which fatigue and exercise intolerance are the dominant complaints (Pratt & Khan, 2016; Pasricha et al., 2021).
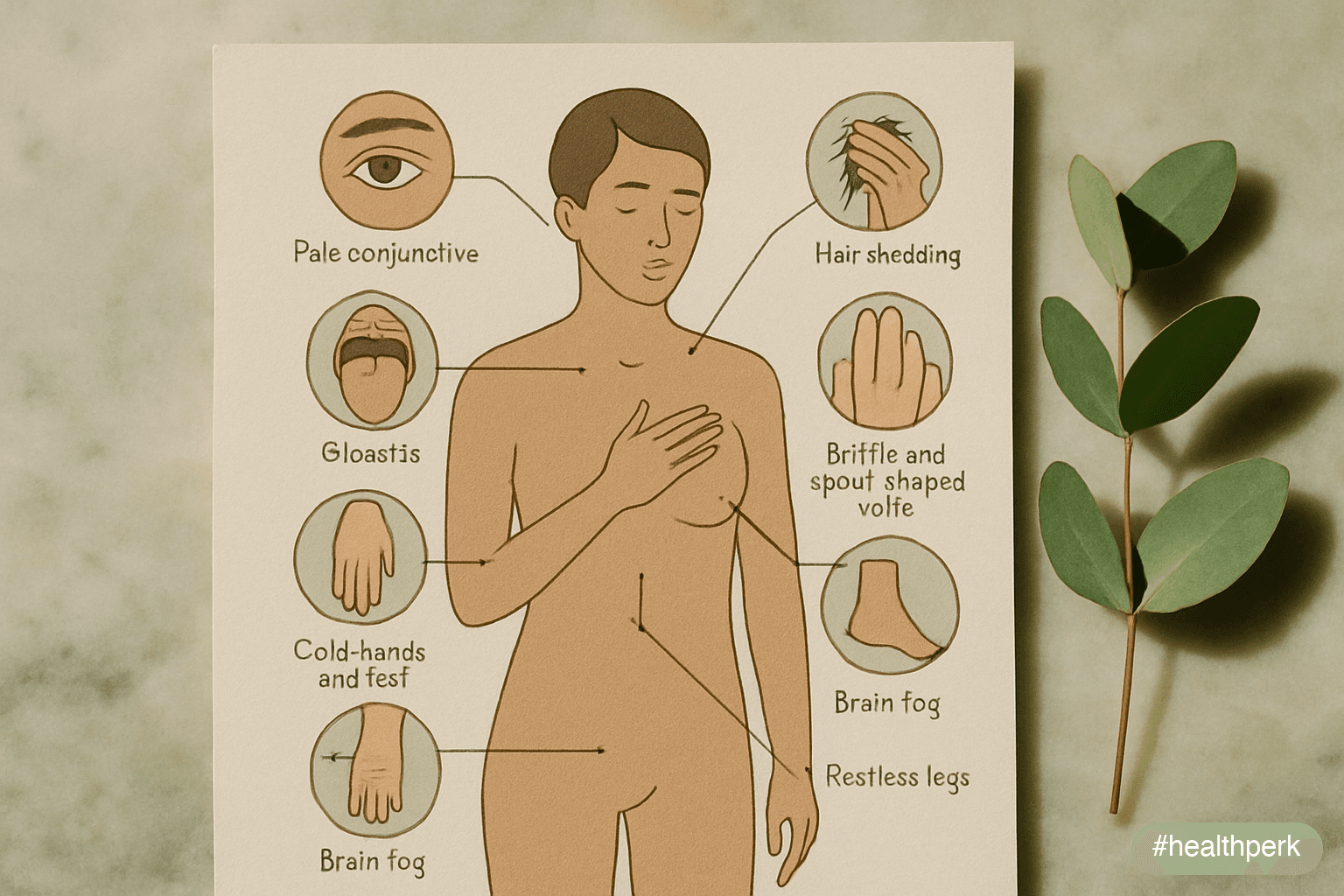
Symptoms in approximate order of how often they appear
- Persistent fatigue disproportionate to activity — flat tiredness across the day, worse with exertion, not fixed by sleep or caffeine. Often the chief complaint that triggers testing.
- Breathlessness on stairs or moderate exertion — appears before resting symptoms; reflects reduced oxygen-carrying capacity.
- Brain fog, reduced concentration, mild memory complaints — frequently dismissed as stress or workload.
- Hair shedding — diffuse, often noticed in the shower or on the brush; ferritin <30–50 ng/mL is a recognized telogen-effluvium driver (Trost et al., 2006).
- Restless legs syndrome (RLS) — uncomfortable urge to move the legs at rest, particularly in the evening. Iron deficiency is one of the most consistent and reversible drivers (Allen et al., 2018).
- Cold hands and feet, exercise intolerance — reduced peripheral oxygen delivery and impaired thermogenesis.
- Pallor of the inner eyelids, palms, and nail beds — useful clinical sign; less reliable in dark skin tones where conjunctival pallor is the best site.
- Brittle, ridged, or spoon-shaped nails (koilonychia) — late sign of chronic iron deficiency.
- Pica — craving and chewing ice (pagophagia), starch, or clay — unusual but highly specific for iron deficiency; resolves within days of replacement.
- Sore or smooth tongue (glossitis), cracks at the corners of the mouth (angular cheilitis) — late signs.
- Heart palpitations, faster resting heart rate — compensatory in anemia.
- Heavy menstrual bleeding noted alongside symptoms — both cause and consequence; deserves OB/GYN evaluation if quality of life is affected.
What is not a reliable sign
Fingernail half-moons, tongue patches, and isolated tiredness without other clues are weak signals. Ferritin testing is what separates iron-driven fatigue from the long list of competing causes (B12 deficiency, vitamin D deficiency, hypothyroidism, sleep apnea, depression).
Iron Deficiency Without Anemia: Why Ferritin Matters More Than Hemoglobin

Body iron is depleted in stages, and symptoms emerge at stage 2 — before hemoglobin falls (Lopez et al., 2016; Pasricha et al., 2021):
- Stage 1 — Iron sufficiency. Ferritin within normal range (women typically 30–200 ng/mL, men 50–300 ng/mL). No symptoms.
- Stage 2 — Iron deficiency without anemia (IDWA). Ferritin falls below ~30 ng/mL. Hemoglobin remains in the normal range. Body has stopped replenishing storage iron but is still meeting oxygen-carrying demand at rest. Fatigue, hair shedding, exercise intolerance, restless legs, brain fog, and cold intolerance all begin here.
- Stage 3 — Iron deficiency anemia (IDA). Ferritin typically <15 ng/mL with low hemoglobin and microcytic, hypochromic red cells on CBC. Full symptom picture, including pallor, palpitations, marked breathlessness.
Why this matters for testing
Hemoglobin alone misses up to a third of symptomatic adults at stage 2 (Pratt & Khan, 2016). The 2026 default is to request ferritin together with a CBC whenever iron deficiency is on the differential — especially in menstruating adults, vegetarians, endurance athletes, and pregnant or postpartum women.
What ferritin number to ask for
- <15 ng/mL: clearly deficient; treat.
- 15–30 ng/mL: deficient by modern criteria; treat if symptoms warrant.
- 30–50 ng/mL: borderline; many symptomatic adults benefit from a trial of replacement, particularly women with hair shedding, restless legs, or postpartum fatigue.
- >50–100 ng/mL: generally adequate for non-pregnant adults; restless-legs specialists often target >75–100 ng/mL when RLS is the primary symptom (Allen et al., 2018).
- Pregnancy: ferritin <30 ng/mL is deficient; routine first-trimester ferritin checking is supported (Pavord et al., 2020).
A trap: ferritin is an acute-phase reactant
Ferritin rises with inflammation, infection, liver disease, alcohol use, and obesity, which can mask iron deficiency. If ferritin looks "okay" but suspicion is high, request transferrin saturation (TSAT) — values below 20% suggest functional iron deficiency even with normal-looking ferritin. C-reactive protein (CRP) helps interpret the picture.
Who Is at Highest Risk in 2026
Iron deficiency is far more common than most other nutritional deficiencies because iron loss and demand fluctuate substantially across the life course. The high-risk groups (Lopez et al., 2016; Pasricha et al., 2021; Pavord et al., 2020):
Menstruating women
Menstrual blood loss is the single largest driver. Heavy menstrual bleeding (HMB) — defined as >80 mL per cycle, soaking through pads or tampons hourly, passing large clots, or periods lasting longer than 7 days — places women in chronic negative iron balance unless intake and absorption keep pace. The prevalence of iron deficiency in menstruating women is consistently 15–30% across population studies, with iron deficiency anemia at 5–10%.
Pregnant and postpartum women
Iron demand approximately doubles during pregnancy, and 30–50% of pregnancies in many regions are complicated by iron deficiency by the third trimester (Pavord et al., 2020). Postpartum iron deficiency frequently persists for months — particularly after surgical delivery, hemorrhage, twin pregnancies, or short inter-pregnancy intervals — and is a major underrecognized cause of postpartum fatigue and mood symptoms.
Vegetarians and vegans
Plant iron (non-heme) absorbs at ~5–12% under typical conditions, compared with ~25% for heme iron from animal sources. Dietary recommendations for vegetarians are approximately 1.8× those for omnivores. Adequate iron status is achievable on plant-based diets but requires intentional pairing with vitamin C–rich foods and attention to polyphenols and phytates that inhibit absorption.
Endurance athletes
Foot-strike hemolysis, increased exercise-induced hepcidin (which blocks iron absorption for 3–6 hours after intense training), sweat losses, and gastrointestinal microbleeding combine to push iron status downward — especially in distance runners, triathletes, and rowers (Sim et al., 2019). Female endurance athletes are doubly affected.
Older adults with new-onset iron deficiency
In adults over 50, new iron deficiency without an obvious dietary cause must trigger a workup for occult gastrointestinal blood loss (colon cancer, gastric ulcer, angiodysplasia, celiac disease). This is non-negotiable; iron supplementation alone without source workup risks delayed diagnosis of colorectal cancer.
Adults with celiac disease, inflammatory bowel disease, or after bariatric surgery
Malabsorption is a frequent cause of treatment-resistant iron deficiency. Celiac serology (tissue transglutaminase IgA) is reasonable in any adult with iron deficiency that fails to respond to oral replacement.
Adults on PPIs long-term
Reduced gastric acid impairs the reduction of ferric iron and inhibits absorption. The effect is modest but cumulative over years.
How Iron Deficiency Is Diagnosed: The Right Panel
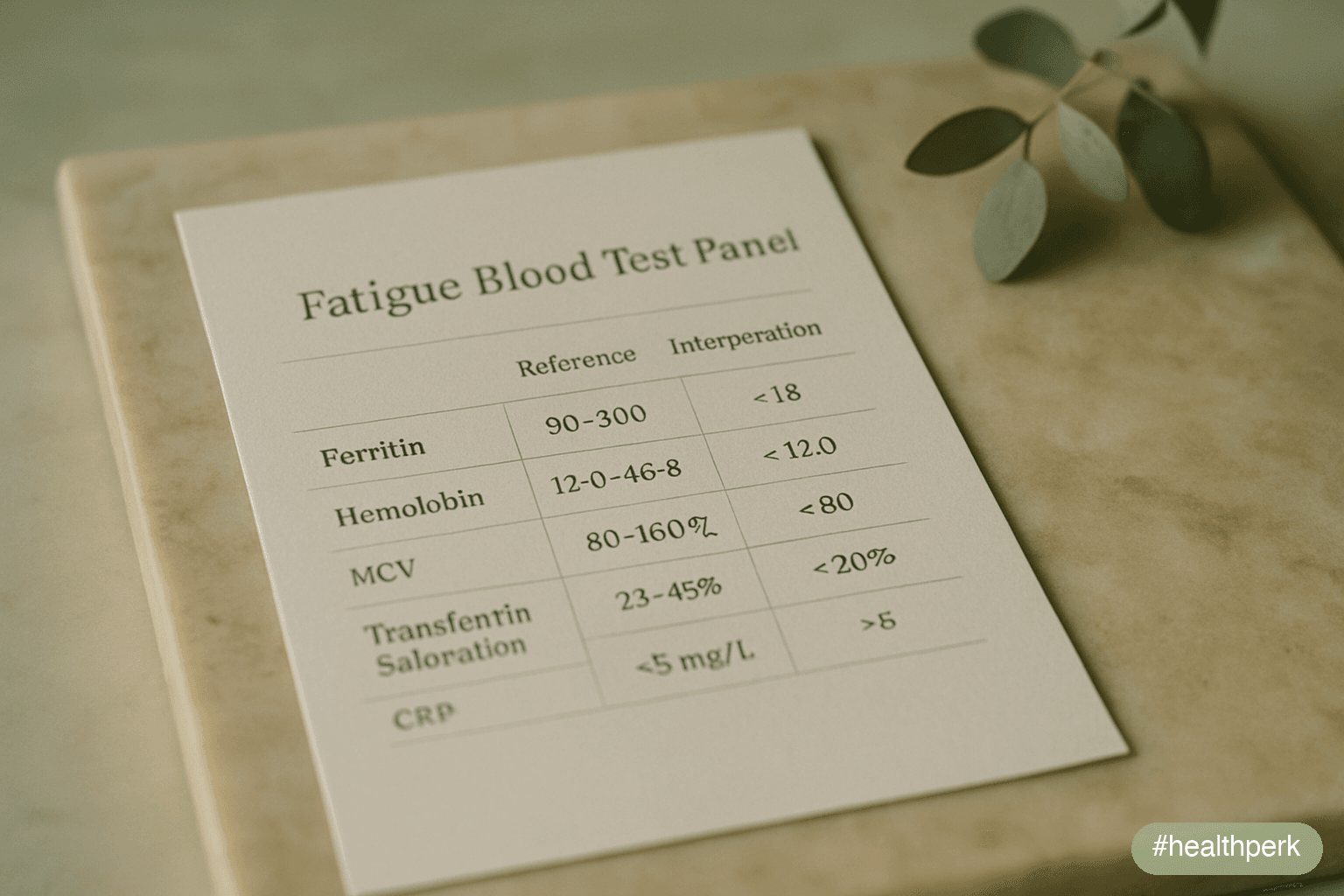
The 2026 default panel for suspected iron deficiency:
- Complete blood count (CBC) with red cell indices — hemoglobin, hematocrit, mean corpuscular volume (MCV), red cell distribution width (RDW). Microcytic, hypochromic anemia (low MCV, low MCH) is the classic pattern, but normocytic anemia and even normal indices are common at early stages.
- Ferritin — the most useful single marker of body iron stores. Interpret in the context of inflammation.
- Transferrin saturation (TSAT) — calculated from serum iron and total iron-binding capacity (TIBC). TSAT <20% supports functional iron deficiency.
- C-reactive protein (CRP) — distinguishes inflammation-related ferritin elevation from genuine sufficiency.
- Reticulocyte hemoglobin content (CHr) — modern, increasingly available marker of recent iron incorporation; particularly useful when ferritin is confounded by inflammation.
Add to the workup based on context
- Tissue transglutaminase IgA (tTG-IgA) for celiac if oral iron fails or iron deficiency recurs.
- Fecal occult blood / colonoscopy in adults >50, or younger adults with weight loss, change in bowel habits, blood in stool, or family history of colorectal cancer.
- OB/GYN evaluation for women with heavy menstrual bleeding.
- Hepcidin (research/specialist setting) when chronic disease anemia is on the differential.
What to skip
Direct-to-consumer "iron status panels" of 20+ markers are usually unnecessary. The five-marker panel above (CBC, ferritin, TSAT, CRP, plus tTG-IgA in resistant cases) covers diagnosis and triages cause efficiently.
Iron Supplements for Fatigue in Women: Dosage, Forms, and What Actually Absorbs
The right answer to iron supplements for fatigue women has changed substantially in the last decade. Two large physiology studies established that high daily oral doses paradoxically reduce absorption by triggering a 24-hour hepcidin spike, and that alternate-day single-dose regimens absorb a larger fraction of the dose with fewer side effects (Stoffel et al., 2017; Moretti et al., 2015). This is the 2026 default for non-emergency replacement.
Standard oral protocol (iron deficiency with or without anemia)
- Dose: 60–120 mg elemental iron, taken as a single morning dose.
- Schedule: every other day, not daily. (Daily dosing remains an option, particularly during pregnancy or where speed matters, but absorption is no better and gastrointestinal side effects are worse.)
- Timing: on an empty stomach if tolerated, ~1 hour before food, with a glass of water and ~100–250 mg vitamin C or a vitamin C–rich food (orange juice, kiwi, strawberries) to enhance non-heme iron uptake.
- Avoid with the dose: coffee, tea, milk, calcium supplements, antacids, and high-fiber foods within ~2 hours (all inhibit absorption).
- Duration: continue for 3 months after ferritin returns to target (>50 ng/mL for general use; ≥75–100 ng/mL in restless-legs syndrome) to refill stores.
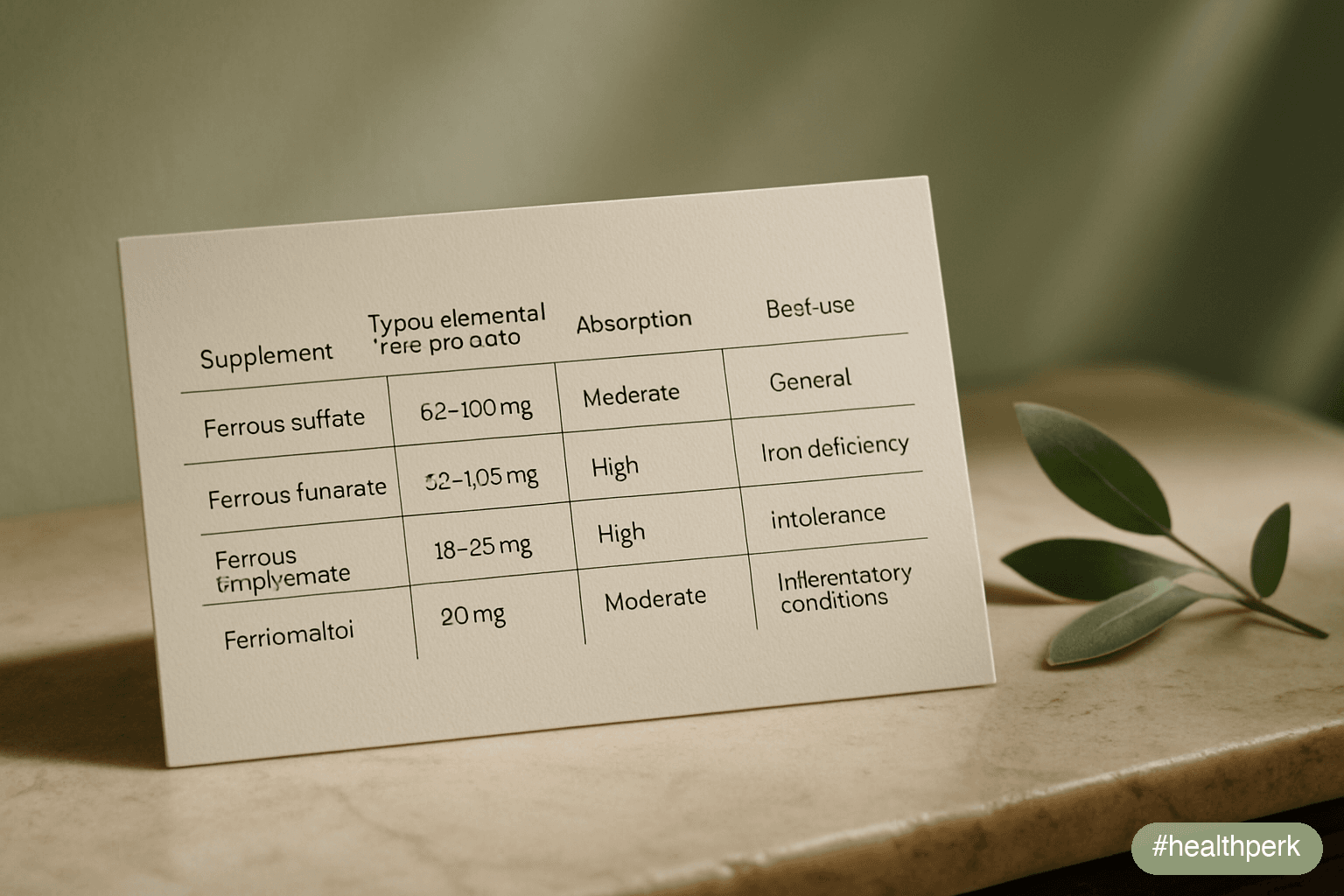
Forms — practical guidance
- Ferrous sulfate (e.g., 325 mg tablet = 65 mg elemental iron): cheapest, most studied, effective. GI side effects (constipation, nausea, dark stools, metallic taste) are the main limiter.
- Ferrous fumarate (~33% elemental iron): equivalent efficacy to sulfate, slightly different side-effect profile; reasonable swap if sulfate is poorly tolerated.
- Ferrous bisglycinate (chelated iron, ~20% elemental iron): better gastrointestinal tolerability in randomized comparisons; absorption appears equivalent at appropriate elemental-iron doses. Often the right starting choice for women with prior intolerance to sulfate.
- Ferric maltol (30 mg twice daily): newer prescription oral option for adults with inflammatory bowel disease or sulfate intolerance; specialist-driven.
- Polysaccharide iron complex: non-ionic; tolerability claims exceed evidence; absorption in head-to-head trials has been mixed.
- Liposomal iron and sucrosomial iron: emerging oral forms with reduced GI side effects; modest evidence base; reasonable for adults who cannot tolerate conventional forms.
- Avoid: "iron-rich" multivitamins for treating deficiency (elemental doses are too low) and herbal "blood tonics" without standardized iron content.
Tracking response
Reticulocyte count rises within 7–10 days; hemoglobin rises ~1 g/dL per 2–4 weeks in iron deficiency anemia; ferritin replenishes over months. Recheck CBC and ferritin at 6–8 weeks, then again at 3–4 months. If ferritin has not risen meaningfully by 8 weeks despite adherence, suspect malabsorption, ongoing blood loss, or non-adherence — and consider intravenous iron.
Practical advice for women specifically
- Time iron replacement to begin immediately after the heaviest menstrual day, not before, to align with the body's natural absorption rebound.
- Pair every dose with vitamin C and separate it from coffee, tea, and dairy by at least 2 hours.
- For women with heavy menstrual bleeding, treat the bleeding (hormonal options, tranexamic acid, evaluation of fibroids/adenomyosis) in parallel with iron replacement — otherwise replacement is a leaky bucket.
- Postpartum: oral iron starting within the first weeks postpartum is appropriate for ferritin <30 ng/mL or symptomatic women; intravenous iron has a clear role after postpartum hemorrhage or in severe deficiency (Pavord et al., 2020).
- Avoid co-prescription with calcium supplements, levothyroxine, fluoroquinolones, and tetracyclines at the same time of day — separate by at least 2 hours.
Food Sources and Absorption Hacks
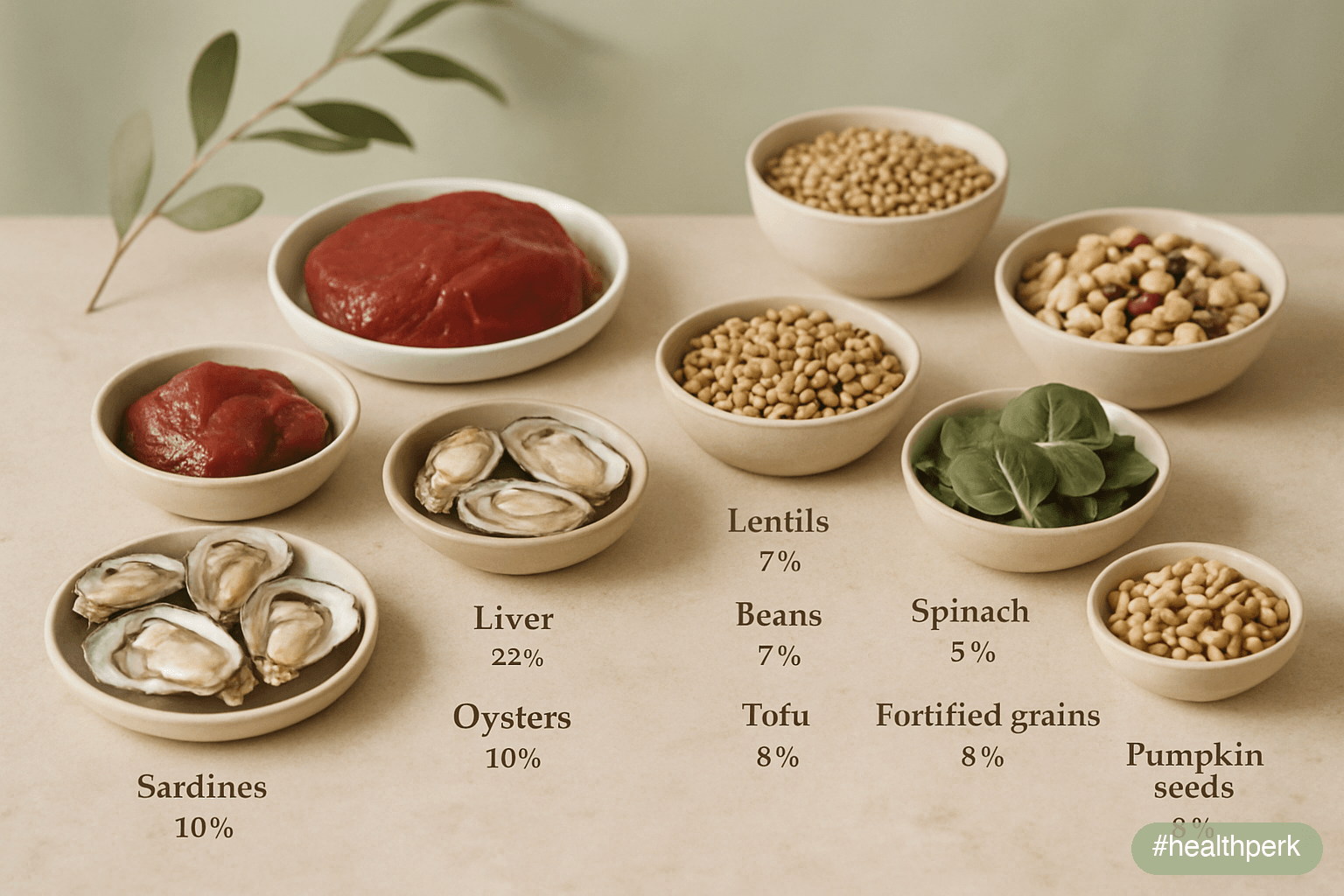
Diet alone rarely corrects established deficiency but is the foundation of long-term iron status.
Heme iron (animal sources, ~15–25% absorption)
- Beef, lamb, and pork (especially organ meats)
- Chicken and turkey dark meat
- Oysters, clams, mussels, sardines, anchovies
- Egg yolks (modest)
Non-heme iron (plant sources, ~5–12% absorption)
- Lentils, chickpeas, kidney beans, white beans
- Tofu and tempeh
- Pumpkin seeds, sesame seeds, hemp hearts, cashews
- Cooked spinach, Swiss chard, beet greens
- Quinoa, fortified breakfast cereals, fortified breads
- Dried apricots, prunes, raisins
- Dark chocolate (modest)
Boosters and blockers
- Boosters: vitamin C in the same meal (citrus, berries, tomatoes, peppers, kiwi), small amounts of meat eaten with plant iron (the "meat factor"), and fermented or sprouted preparations of grains and legumes (reduces phytate).
- Blockers: coffee and tea polyphenols, calcium (dairy and supplements), phytates in unsoaked legumes and whole grains, oxalates (spinach without vitamin C), and certain medications (PPIs, antacids).
- Practical move: separate coffee/tea from iron-rich meals by ~1–2 hours; keep dairy out of iron-rich meals; finish meals with vitamin C–rich fruit.
A note on cast-iron cookware
Cooking acidic foods (tomato sauces) in cast iron does increase the iron content of the food, but the contribution is modest and inconsistent compared with diet and supplementation; treat as a small bonus, not a strategy.
When Oral Iron Fails: Intravenous Iron in 2026
Intravenous (IV) iron has moved from a niche option to a mainstream second-line choice in 2026. Indications (Auerbach & Schrier, 2017; Pavord et al., 2020):
- Documented oral iron intolerance (severe GI side effects despite alternate-day dosing and form changes)
- Inadequate response to oral iron after 8 weeks of confirmed adherence
- Inflammatory bowel disease (active or recent flare), as oral iron exacerbates inflammation
- Severe iron deficiency anemia requiring rapid correction
- Chronic kidney disease, heart failure with iron deficiency, oncology supportive care
- Postpartum hemorrhage with severe anemia
- Pre-operative anemia within 4–6 weeks of major surgery
Current preparations
Modern IV iron formulations (ferric carboxymaltose, ferric derisomaltose, iron sucrose, low-molecular-weight iron dextran) allow large total-dose infusions in 1–2 visits with low rates of serious reactions when administered in appropriate clinical settings. Hypophosphatemia is a recognized side effect of ferric carboxymaltose and warrants monitoring after repeated dosing.
IV iron is not a cosmetic or wellness intervention; it requires clinical indication, monitoring, and follow-up. It is, however, dramatically underused for postpartum women, women with refractory heavy menstrual bleeding, and adults with IBD — populations where oral failure is common and quality-of-life improvement after IV correction is substantial.
Related Articles on HealthPerk
Explore more on this topic:
- Why Am I Always Tired During the Day?
- Best Supplements for Energy and Fatigue
- B12 Deficiency Symptoms and Fatigue
- How to Boost Energy Naturally Without Caffeine
- Foods That Boost Energy
Frequently Asked Questions
What are the early iron deficiency fatigue symptoms before anemia shows up?
The earliest signs are persistent fatigue disproportionate to activity, breathlessness on stairs, brain fog, diffuse hair shedding, restless legs at night, cold hands and feet, and reduced exercise tolerance — frequently with a normal or near-normal hemoglobin. Pica (especially ice cravings), brittle nails, and pallor of the inner eyelids appear as deficiency deepens. Because hemoglobin can stay normal for months while body iron stores fall, the right test is a CBC plus ferritin together, not hemoglobin alone. Ferritin below 30 ng/mL with symptoms is enough to justify treatment in most adults.
What ferritin level is too low?
Modern thresholds: ferritin below 15 ng/mL is clearly deficient; 15–30 ng/mL is deficient by 2026 criteria and should be treated when symptoms are present; 30–50 ng/mL is borderline and a trial of replacement is reasonable in women with hair shedding, postpartum fatigue, or restless legs; restless legs syndrome specialists often target >75–100 ng/mL. Ferritin rises with inflammation, infection, alcohol use, and liver disease, so a normal-looking ferritin paired with a transferrin saturation under 20% can still indicate functional iron deficiency.
Can I have iron deficiency without anemia?
Yes — this is the most common scenario in fatigued adults and is often missed. Body iron depletes in stages: ferritin falls first, hemoglobin stays normal initially, and full anemia appears only after stores are exhausted. Symptoms (fatigue, breathlessness, hair shedding, restless legs, brain fog, exercise intolerance) typically begin at the iron deficiency without anemia stage, when ferritin drops below ~30 ng/mL. Routine "normal CBC, you're fine" reassurance misses this entirely. Ask for ferritin specifically.
Which iron supplements for fatigue women absorb best?
The 2026 evidence-based protocol: 60–120 mg of elemental iron taken every other day as a single morning dose, on an empty stomach, with vitamin C, separated from coffee, tea, dairy, and calcium supplements by at least 2 hours. Alternate-day dosing absorbs more total iron than daily dosing with fewer side effects, because high daily doses trigger a 24-hour hepcidin spike that blocks the next day's absorption. Ferrous sulfate is cheapest and well-studied; ferrous bisglycinate is better tolerated for women who get gut side effects from sulfate.
How long until iron supplements improve fatigue?
Reticulocyte count rises within 7–10 days, hemoglobin improves by about 1 g/dL every 2–4 weeks if anemic, and ferritin refills over months. Subjective fatigue improvement is often noticeable within 2–4 weeks, particularly in iron deficiency without anemia. Continue treatment for 3 months after ferritin reaches target (typically >50 ng/mL; ≥75–100 ng/mL for restless legs syndrome). If there is no meaningful response by 8 weeks despite good adherence, suspect malabsorption (consider celiac testing), ongoing blood loss, or the need for intravenous iron.
Why do iron pills make me nauseous and constipated?
Conventional ferrous sulfate at high daily doses delivers a large bolus of free iron to the upper gut, which generates oxidative stress in the intestinal mucosa, irritates the stomach, and slows transit. Three changes help: switch to alternate-day dosing (proven to absorb at least as well with fewer side effects), try ferrous bisglycinate or ferrous fumarate, and take with vitamin C and a small amount of food if empty-stomach dosing is intolerable. Dark stools are normal and not a sign of bleeding. If side effects persist, intravenous iron is a reasonable next step.
Should men take iron supplements for fatigue?
Generally no — without confirmed deficiency on bloodwork. Men accumulate iron more readily than menstruating women and are at risk for iron overload from unnecessary supplementation, especially if undiagnosed hereditary hemochromatosis is present. New iron deficiency in a man (or in a postmenopausal woman) must trigger a workup for occult gastrointestinal blood loss, including colonoscopy and consideration of celiac disease, rather than empirical iron supplementation. Test before treating.
Do I need intravenous iron, or is oral enough?
Oral iron is first-line and sufficient for most adults. Intravenous iron is indicated when oral iron fails after 8 weeks of confirmed adherence, when oral iron is not tolerated despite form and dose changes, in active inflammatory bowel disease, in severe anemia requiring rapid correction, in postpartum hemorrhage, in pre-operative anemia within 4–6 weeks of major surgery, and in chronic kidney or heart disease with iron deficiency. Modern formulations (ferric carboxymaltose, ferric derisomaltose) deliver large total-dose infusions in 1–2 visits with low serious-reaction rates.
This article is for informational purposes only and does not constitute medical advice. New-onset iron deficiency in men, postmenopausal women, or adults over 50 requires a workup for gastrointestinal blood loss, including colonoscopy. Severe anemia, breathlessness at rest, chest pain, fainting, or symptoms in pregnancy require prompt professional evaluation. Do not begin high-dose iron therapy without confirmed deficiency on bloodwork, particularly if hereditary hemochromatosis runs in the family. Consult a qualified healthcare provider before making significant changes to medication, supplementation, diet, or exercise, especially if you are pregnant or breastfeeding or have a chronic medical condition. Individual results may vary.
About the author The HealthPerk Editorial Team reviews internal-medicine, hematology, obstetrics, sports medicine, and nutrition literature through evidence synthesis cross-referenced with peer-reviewed clinical trials and current professional-society guidelines. How we review →
References
Pasricha, S. R., Tye-Din, J., Muckenthaler, M. U., & Swinkels, D. W. (2021). Iron deficiency. The Lancet, 397(10270), 233–248. https://doi.org/10.1016/S0140-6736(20)32594-0
Supports: ferritin thresholds, staged depletion, iron deficiency without anemia, modern diagnostic approach
Lopez, A., Cacoub, P., Macdougall, I. C., & Peyrin-Biroulet, L. (2016). Iron deficiency anaemia. The Lancet, 387(10021), 907–916. https://doi.org/10.1016/S0140-6736(15)60865-0
Supports: epidemiology, clinical presentation, oral iron replacement framework
Pratt, J. J., & Khan, K. S. (2016). Non-anaemic iron deficiency — a disease looking for recognition of diagnosis: a systematic review. European Journal of Haematology, 96(6), 618–628. https://doi.org/10.1111/ejh.12645
Supports: iron deficiency without anemia as a symptomatic clinical entity
Stoffel, N. U., Cercamondi, C. I., Brittenham, G., Zeder, C., Geurts-Moespot, A. J., Swinkels, D. W., Moretti, D., & Zimmermann, M. B. (2017). Iron absorption from oral iron supplements given on consecutive versus alternate days and as single morning doses versus twice-daily split dosing in iron-depleted women: two open-label, randomised controlled trials. The Lancet Haematology, 4(11), e524–e533. https://doi.org/10.1016/S2352-3026(17)30182-5
Supports: alternate-day dosing absorbs more total iron with fewer side effects
Moretti, D., Goede, J. S., Zeder, C., Jiskra, M., Chatzinakou, V., Tjalsma, H., Melse-Boonstra, A., Brittenham, G., Swinkels, D. W., & Zimmermann, M. B. (2015). Oral iron supplements increase hepcidin and decrease iron absorption from daily or twice-daily doses in iron-depleted young women. Blood, 126(17), 1981–1989. https://doi.org/10.1182/blood-2015-05-642223
Supports: hepcidin response to high daily oral iron doses
Pavord, S., Daru, J., Prasannan, N., Robinson, S., Stanworth, S., & Girling, J. (2020). UK guidelines on the management of iron deficiency in pregnancy. British Journal of Haematology, 188(6), 819–830. https://doi.org/10.1111/bjh.16221
Supports: pregnancy ferritin thresholds, postpartum management, IV iron indications
Auerbach, M., & Schrier, S. (2017). Treatment of iron deficiency is getting trendy. The Lancet Haematology, 4(11), e500–e501. https://doi.org/10.1016/S2352-3026(17)30194-1
Supports: modern indications and uptake of intravenous iron
Allen, R. P., Picchietti, D. L., Auerbach, M., Cho, Y. W., Connor, J. R., Earley, C. J., Garcia-Borreguero, D., Kotagal, S., Manconi, M., Ondo, W., Ulfberg, J., & Winkelman, J. W. (2018). Evidence-based and consensus clinical practice guidelines for the iron treatment of restless legs syndrome/Willis-Ekbom disease in adults and children: an IRLSSG task force report. Sleep Medicine, 41, 27–44. https://doi.org/10.1016/j.sleep.2017.11.1126
Supports: ferritin targets and iron therapy in restless legs syndrome
Sim, M., Garvican-Lewis, L. A., Cox, G. R., Govus, A., McKay, A. K. A., Stellingwerff, T., & Peeling, P. (2019). Iron considerations for the athlete: a narrative review. European Journal of Applied Physiology, 119(7), 1463–1478. https://doi.org/10.1007/s00421-019-04157-y
Supports: exercise-induced hepcidin, foot-strike hemolysis, athlete iron loss
Trost, L. B., Bergfeld, W. F., & Calogeras, E. (2006). The diagnosis and treatment of iron deficiency and its potential relationship to hair loss. Journal of the American Academy of Dermatology, 54(5), 824–844. https://doi.org/10.1016/j.jaad.2005.11.1104
Supports: ferritin–telogen effluvium relationship and hair-loss thresholds
Camaschella, C. (2019). Iron deficiency. Blood, 133(1), 30–39. https://doi.org/10.1182/blood-2018-05-815944
Supports: pathophysiology of iron deficiency and hepcidin regulation
Kassebaum, N. J., GBD 2013 Anemia Collaborators. (2016). The global burden of anemia. Hematology/Oncology Clinics of North America, 30(2), 247–308. https://doi.org/10.1016/j.hoc.2015.11.002
Supports: global prevalence of iron deficiency anemia, demographic distribution
Frequently Asked Questions
What are the early iron deficiency fatigue symptoms before anemia shows up?
The earliest signs are persistent fatigue disproportionate to activity, breathlessness on stairs, brain fog, diffuse hair shedding, restless legs at night, cold hands and feet, and reduced exercise tolerance — frequently with a normal or near-normal hemoglobin. Pica (especially ice cravings), brittle nails, and pallor of the inner eyelids appear as deficiency deepens. Because hemoglobin can stay normal for months while body iron stores fall, the right test is a CBC plus ferritin together, not hemoglobin alone. Ferritin below 30 ng/mL with symptoms is enough to justify treatment in most adults.
What ferritin level is too low?
Ferritin below 15 ng/mL is clearly deficient; 15–30 ng/mL is deficient by 2026 criteria and should be treated when symptoms are present; 30–50 ng/mL is borderline and a trial of replacement is reasonable in women with hair shedding, postpartum fatigue, or restless legs; restless legs syndrome specialists often target greater than 75–100 ng/mL. Ferritin rises with inflammation, infection, alcohol use, and liver disease, so a normal-looking ferritin paired with a transferrin saturation under 20% can still indicate functional iron deficiency.
Can I have iron deficiency without anemia?
Yes — this is the most common scenario in fatigued adults and is often missed. Body iron depletes in stages: ferritin falls first, hemoglobin stays normal initially, and full anemia appears only after stores are exhausted. Symptoms (fatigue, breathlessness, hair shedding, restless legs, brain fog, exercise intolerance) typically begin at the iron deficiency without anemia stage when ferritin drops below ~30 ng/mL. Routine normal-CBC reassurance misses this entirely. Ask for ferritin specifically.
Which iron supplements for fatigue women absorb best?
The 2026 evidence-based protocol: 60–120 mg of elemental iron taken every other day as a single morning dose, on an empty stomach, with vitamin C, separated from coffee, tea, dairy, and calcium supplements by at least 2 hours. Alternate-day dosing absorbs more total iron than daily dosing with fewer side effects, because high daily doses trigger a 24-hour hepcidin spike that blocks the next day's absorption. Ferrous sulfate is cheapest and well-studied; ferrous bisglycinate is better tolerated for women who get gut side effects from sulfate.
How long until iron supplements improve fatigue?
Reticulocyte count rises within 7–10 days, hemoglobin improves by about 1 g/dL every 2–4 weeks if anemic, and ferritin refills over months. Subjective fatigue improvement is often noticeable within 2–4 weeks, particularly in iron deficiency without anemia. Continue treatment for 3 months after ferritin reaches target. If there is no meaningful response by 8 weeks despite good adherence, suspect malabsorption (consider celiac testing), ongoing blood loss, or the need for intravenous iron.
Why do iron pills make me nauseous and constipated?
Conventional ferrous sulfate at high daily doses delivers a large bolus of free iron to the upper gut, generates oxidative stress in the mucosa, irritates the stomach, and slows transit. Three changes help: switch to alternate-day dosing (proven to absorb at least as well with fewer side effects), try ferrous bisglycinate or ferrous fumarate, and take with vitamin C and a small amount of food if empty-stomach dosing is intolerable. Dark stools are normal. If side effects persist, intravenous iron is a reasonable next step.
Should men take iron supplements for fatigue?
Generally no — without confirmed deficiency on bloodwork. Men accumulate iron more readily than menstruating women and are at risk for iron overload from unnecessary supplementation, especially if undiagnosed hereditary hemochromatosis is present. New iron deficiency in a man or in a postmenopausal woman must trigger a workup for occult gastrointestinal blood loss, including colonoscopy and consideration of celiac disease, rather than empirical iron supplementation. Test before treating.
Do I need intravenous iron, or is oral enough?
Oral iron is first-line and sufficient for most adults. Intravenous iron is indicated when oral iron fails after 8 weeks of confirmed adherence, when oral iron is not tolerated despite form and dose changes, in active inflammatory bowel disease, in severe anemia requiring rapid correction, in postpartum hemorrhage, in pre-operative anemia within 4–6 weeks of major surgery, and in chronic kidney or heart disease with iron deficiency. Modern formulations deliver large total-dose infusions in 1–2 visits with low serious-reaction rates.
More from Supplements


