
Best Supplements for Focus and Concentration: A 2026 Evidence-Based Guide
Best Supplements for Focus and Concentration: A 2026 Evidence-Based Guide
By the HealthPerk Editorial Team · Last updated: May 2026
Quick Answer
What are the best supplements for focus and concentration in 2026?
The honest short answer is that supplements help most when they correct an underlying deficiency, and help much less when they are added on top of an already adequate diet. The two interventions with the strongest evidence — and the lowest risk — are correcting iron, vitamin B12, vitamin D, and omega-3 status when measurably low, and adding L-theanine alongside moderate caffeine for acute focus sessions. Almost everything else falls into a moderate-evidence or weak-evidence tier that may help some people and not others, with effect sizes smaller than sleep, exercise, or environment design.
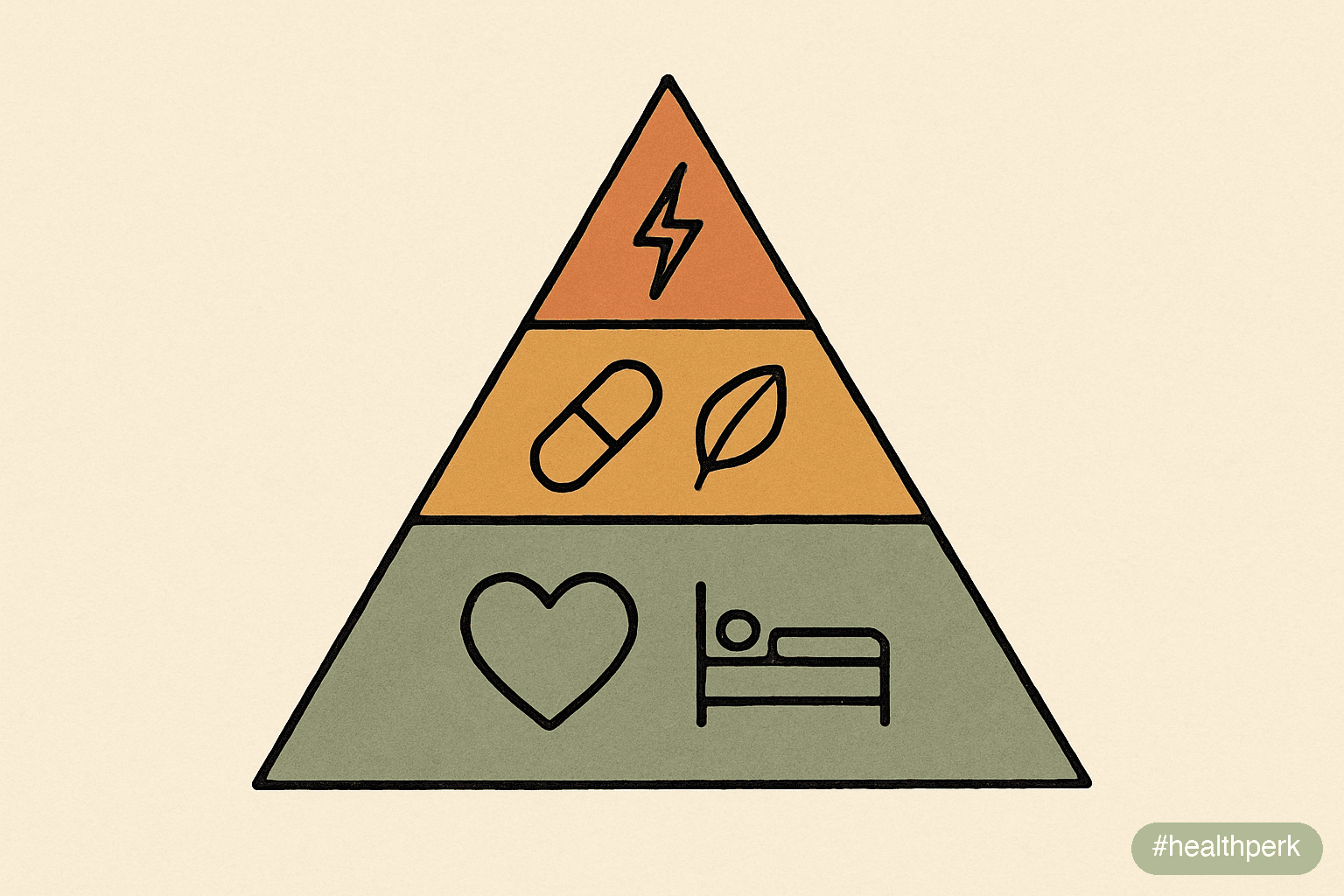
A practical tiering for 2026:
| Tier | Examples | Evidence | When to use |
|---|---|---|---|
| 1 — Correct deficiencies | Iron, B12, vitamin D, omega-3 | Strong when low | After a blood test shows low status |
| 2 — Reliable modest effect | L-theanine + caffeine, creatine | Moderate–strong | For specific acute or training needs |
| 3 — Mixed, individual response | Rhodiola, bacopa, ginkgo, lion's mane | Moderate, contested | Trial for 8–12 weeks with one variable changed |
| 4 — Marketed but thin evidence | Most "nootropic stacks", proprietary blends | Weak | Skip unless willing to spend on uncertainty |

Best supplements for focus and concentration is one of the most searched health topics of 2026, and also one of the most over-promised. Almost every product page implies that the right capsule will deliver clearer thinking, faster recall, and longer attention spans — outcomes that, in reality, depend much more heavily on sleep, blood-sugar regulation, and screen environment than on any pill. The supplement layer is real and sometimes meaningful, but it works best when it sits on top of those foundations, not as a substitute for them.
This guide is organized as a tiered review rather than a ranked list, because tiering is honest about uncertainty. A supplement that reliably fixes a B12 deficiency belongs in a different category than one that might improve memory after twelve weeks. The 2026 literature, including updated Cochrane reviews and meta-analyses through 2024–2025, supports this kind of categorical thinking and warns against the "more is better" stacking that has become common in online communities.
Table of Contents
- Best Supplements for Focus and Concentration in Adults
- Supplements for Brain Fog: What the Evidence Actually Shows
- Vitamins for Memory and Focus: The Deficiency-First Framework
- Supplements for Cognitive Function: A Tiered View
- Supplements for Mental Clarity: Daily Use vs Acute Use
- Supplements for Students Focus: What Is Reasonable Before Exams
- Frequently Asked Questions
- References
Best Supplements for Focus and Concentration in Adults
Best supplements for focus and concentration adults ask for is rarely the same as what they actually need. The most common request is for "something to take in the morning" that will produce noticeable mental sharpness within an hour. Outside of caffeine, almost nothing reliably does this on a same-day basis. The interventions with the largest within-person effect on focus operate over weeks to months, by correcting underlying biology rather than acutely altering it.
The honest hierarchy for adults:
- First: blood test before supplementing. Ferritin, vitamin B12, vitamin D (25-OH), and a complete blood count are the four most common tests that surface fixable causes of poor focus. Reviews of iron and cognition have found that iron deficiency without anemia produces measurable cognitive symptoms that resolve with iron repletion. Skipping this step often means buying expensive supplements while ignoring a $40 fix.
- Second: correct what is low. Replacement doses (not maintenance doses) for documented deficiencies, taken consistently for at least 8–12 weeks. Re-test before deciding whether the supplement is "working."
- Third: layer evidence-backed staples. Omega-3 (EPA + DHA) at roughly 1–2 grams daily, vitamin D at the dose needed to bring levels into the 30–50 ng/mL range, and creatine monohydrate at 3–5 grams daily for those who tolerate it. These three have the most consistent evidence base across multiple meta-analyses through 2025.
- Fourth: trial one acute-use compound at a time. L-theanine + moderate caffeine for focus sessions, or rhodiola for stress-driven mental fatigue. One variable at a time, for 4–8 weeks, with notes — otherwise the signal is indistinguishable from week-to-week variability.
The single most common mistake is starting a five-supplement stack on the same day, feeling slightly better for a week, and then losing the benefit by week three without being able to tell which ingredient (if any) was responsible. Sequential trials are unromantic but produce real knowledge.
What does not appear on this list and why
- Proprietary "nootropic blends" that list a dozen ingredients without per-ingredient doses. The dose disclosure is the first signal of quality; its absence is a near-certain sign that effective doses are not present.
- Supplements promising "10x focus" or "limitless" language. No supplement in the 2026 evidence base produces that magnitude of effect. The language alone is reason to skip.
- Combinations that include stimulants beyond caffeine (such as DMHA, synephrine, or undisclosed amphetamine analogs) — these have appeared in recalled products multiple times in the last five years and carry cardiovascular risk.
Supplements for Brain Fog: What the Evidence Actually Shows
Supplements for brain fog is a search that has more than doubled in volume since 2022, driven partly by post-viral cognitive symptoms and partly by the steady rise in chronic stress and poor sleep. Brain fog is not a diagnosis — it is a symptom cluster (slow thinking, word-finding difficulty, fatigue, mild forgetfulness) that has multiple distinct underlying drivers. The supplement that helps depends entirely on which driver is present.
The major drivers worth identifying first:
- Nutrient deficiencies (iron, B12, vitamin D, thiamine in heavy alcohol users).
- Sleep debt or sleep apnea. No supplement compensates for chronic short or fragmented sleep.
- Post-viral or post-Covid cognitive symptoms. Reviews of long-Covid cognitive sequelae have described persistent cognitive symptoms in a subset of post-Covid patients lasting beyond 12 weeks, with mechanisms that include neuroinflammation and autonomic dysfunction.
- Perimenopause and menopause. Estradiol fluctuation produces measurable cognitive changes in many women between roughly 40 and 55; this is real biology, not imagination.
- Medication side effects. Many sleep aids, antihistamines, and anticholinergic medications produce brain-fog-like symptoms.
- Chronic stress and HPA-axis dysregulation. Persistent high cortisol impairs hippocampal function and executive performance.
Supplements for brain fog that work — and the honest qualifiers
Supplements for brain fog that work consistently in research, when matched to the right driver, are a short list:
- Iron, when ferritin is low. Iron repletion (typically with iron bisglycinate or ferrous sulfate, taken with vitamin C, not with calcium or coffee) commonly resolves brain-fog symptoms within 6–12 weeks in low-ferritin adults.
- Vitamin B12, when low or low-normal. Sublingual methylcobalamin or oral cyanocobalamin at 1,000 mcg daily corrects deficiency in most adults; in those with absorption issues, injections may be needed.
- Vitamin D, when 25-OH levels are below 30 ng/mL. Repletion doses (typically 2,000–5,000 IU daily) for 8–12 weeks, then maintenance.
- Omega-3 (EPA + DHA), at meaningful doses. Meta-analyses of omega-3 trials have found that EPA-predominant formulations at 1–2 g/day produce modest improvements in cognitive and mood symptoms in adults with depression-related cognitive complaints.
- Magnesium glycinate, particularly when sleep is poor. Effects on focus are indirect, mediated through better sleep.
What does not work consistently for brain fog: high-stimulant "energy" supplements (these mask fatigue without addressing cause), generic multivitamins at sub-therapeutic doses, and most proprietary "brain support" blends. For post-Covid cognitive symptoms specifically, no single supplement has emerged from the 2026 literature as a clear treatment; the most useful intervention package remains pacing, gradual reconditioning, sleep optimization, and treatment of any identified deficiencies.
Vitamins for Memory and Focus: The Deficiency-First Framework
Vitamins for memory and focus are most effective when they correct a deficiency and least effective when they are added to an already-replete diet. The deficiency-first framework is the rule almost universally supported by the 2026 evidence: vitamins produce robust cognitive benefits when levels are low, and modest-to-no benefit when levels are normal. This is unromantic but important — it means the question is not "which vitamin should I take" but "which vitamin am I likely to be low in, and is that worth testing."
The four vitamins worth focused attention:
- Vitamin B12 (cobalamin). Required for myelin synthesis and neurotransmitter production. Deficiency produces a recognizable syndrome of slow thinking, fatigue, paresthesias, and, if severe, memory loss. Strict vegetarians and vegans, adults over 60, people on metformin, and people on long-term acid suppressants are at elevated risk. Serum B12 below 300 pg/mL is suspicious; methylmalonic acid is a more sensitive marker.
- Folate (vitamin B9). Works with B12 in one-carbon metabolism. Most diets with leafy greens or fortified grains provide adequate folate, but some adults remain marginal. Folate without sufficient B12 can be problematic, which is why B12 status should be checked before high-dose folate supplementation.
- Vitamin D (cholecalciferol). Receptors throughout the brain; deficiency is associated with cognitive symptoms and mood changes in observational studies. Repletion in deficient adults produces consistent symptom improvement; supplementation in already-replete adults shows little or no cognitive benefit.
- Thiamine (vitamin B1). Critical for glucose metabolism in neurons. Deficiency is uncommon in well-fed adults but appears in heavy alcohol users, post-bariatric-surgery patients, and people with chronic vomiting; symptoms can include profound cognitive impairment.
What about a high-dose B-complex "just in case"?
A daily B-complex at moderate doses is low-risk and reasonable for adults whose diets are inconsistent, who are on metformin, or who follow plant-based eating patterns. Megadoses (high-dose B6 in particular) carry actual risk — chronic high B6 intake has been linked to peripheral neuropathy. Moderate, food-form doses are the safer default.
Vitamin E, C, and "antioxidant" packs
The evidence that high-dose antioxidant vitamins prevent or treat cognitive decline is weak; some meta-analyses have suggested neutral or slightly negative effects of high-dose vitamin E supplementation. Antioxidants from food (berries, leafy greens, nuts, fish) consistently associate with better cognitive outcomes; isolated antioxidant pills do not replicate that effect.
Supplements for Cognitive Function: A Tiered View
Supplements for cognitive function vary by an order of magnitude in evidence quality. Lumping them together — as most product pages do — obscures the fact that some compounds have decades of replicated trials behind them while others rest on a handful of small studies funded by their manufacturers. The 2026 tiered view, drawing on Cochrane reviews and major meta-analyses through 2025:
Tier 1 — Strongest evidence
- Omega-3 (EPA + DHA). Multiple meta-analyses support modest improvements in mood, attention, and processing speed, particularly in adults with low baseline intake of oily fish. EPA-predominant formulations at 1–2 g/day are the most consistently supported.
- Creatine monohydrate. A 2023 meta-analysis in Nutrition Reviews (Prokopidis et al.) pooling randomized trials found measurable improvements in short-term memory and reasoning, particularly in vegetarians, sleep-deprived adults, and older adults. Standard dose 3–5 g/day.
- Caffeine + L-theanine. A combination repeatedly shown in controlled studies to produce sharper, less anxious focus than caffeine alone. Typical effective ratio is roughly 100 mg caffeine to 200 mg L-theanine.
Tier 2 — Moderate evidence, individual response
- Rhodiola rosea. Adaptogen with reasonable evidence for stress-related mental fatigue, particularly in burnout and shift-work contexts. Effect size is modest and not universal.
- Bacopa monnieri. Best evidence is for memory after 8–12 weeks of consistent use, not for acute effects. Variable response across individuals.
- Ginkgo biloba. Older literature suggested cognitive benefits in mild cognitive impairment; more recent trials in healthy adults have been less impressive. Mostly neutral in current 2026 meta-analyses.
- Lion's mane (Hericium erinaceus). Promising early evidence, including small randomized trials reporting short-term cognitive performance improvements, but the total trial base remains small and many studies are short.
Tier 3 — Limited or contested evidence
- Phosphatidylserine, citicoline, alpha-GPC. Some positive trials, often industry-funded, with smaller and less consistent effects in independent replications.
- Acetyl-L-carnitine. Mixed; some evidence in older adults with mild cognitive impairment, much less in healthy adults.
- Nootropics from the racetam family (piracetam, etc.). Variable evidence; regulatory status varies by country.
Tier 4 — Marketing, not medicine
Proprietary blends with undisclosed doses, "limitless"-style products, and stacks built around influencer endorsement rather than published data. These are not necessarily harmful, but their cost-to-evidence ratio is poor.
The single most useful action for anyone shopping the cognitive-supplement space in 2026 is to ignore Tier 4 entirely, choose at most one Tier 2 supplement to trial at a time, and ensure Tier 1 staples are already in place.
Supplements for Mental Clarity: Daily Use vs Acute Use

Supplements for mental clarity are most useful when their daily-use and acute-use roles are kept separate. A supplement intended to maintain background cognitive function over months is rarely the same one you would reach for before a 90-minute focused work block. Confusing the two leads to disappointment in both directions.
The daily-use category
Daily-use supplements work by maintaining adequate substrate, reducing inflammation, or correcting a slow-developing deficiency. They produce no perceptible same-day effect. Effects accumulate over weeks. The category includes:
- Omega-3 (EPA + DHA), 1–2 g daily
- Vitamin D at the dose needed to maintain 25-OH levels of 30–50 ng/mL
- A moderate-dose B-complex when diet is irregular
- Magnesium glycinate in the evening for sleep-mediated cognitive benefits
- Creatine monohydrate 3–5 g daily for those who tolerate it
The key is consistency. Skipping daily-use supplements three days a week produces inconsistent serum levels and inconsistent results. Either commit to daily use for 8–12 weeks before evaluating, or do not start.
The acute-use category
Acute-use compounds operate on a same-day timescale and are paired with specific focus tasks. The category is narrower and the evidence is stronger:
- L-theanine + caffeine. The most reliable acute combination for focused work. Typical use: 100 mg caffeine + 200 mg L-theanine, 30 minutes before the task.
- Caffeine alone. Well-studied for vigilance and reaction time, but for sustained focus tasks, L-theanine reduces caffeine's jittery edge without blunting the alerting effect.
- Rhodiola, in some individuals. Particularly for fatigue-driven mental dullness, taken 30–60 minutes before the task.
A useful frame: acute-use compounds are for sharpening available focus. They cannot manufacture focus that is structurally impossible — through poor sleep, intense anxiety, or environmental fragmentation. Layering an acute compound on top of unaddressed structural problems is one of the most common failure modes.
What is not in either category
A surprising number of widely marketed "mental clarity" products do not fit either daily or acute use because their dosing is wrong for both — too low to produce daily effects, too slow-acting for acute effects. The dose disclosure on the label is, again, the best signal of whether a product is serious.
Supplements for Students Focus: What Is Reasonable Before Exams
Supplements for students focus is a search driven mostly by exam season anxiety, and it is the category where overreach is most common. Students are often willing to try almost anything in the week before a major exam — which is precisely the wrong time to introduce new substances. Stimulant exposure (including high-dose caffeine, energy drinks, and prescription stimulants used without diagnosis) is associated with sleep disruption, performance crashes, and rare cardiac events.
The reasonable framework, for student-aged adults (over 18) and with parental supervision for minors:
- Sleep is the highest-leverage "supplement." A 2019 Annual Review of Psychology synthesis confirmed that a full night of sleep after study materially improves retention compared with cramming followed by short sleep. No supplement substitutes for this.
- Hydration. Mild dehydration (2% body water loss) measurably impairs cognitive performance. A water bottle on the desk is cheaper and more effective than most supplements.
- Moderate caffeine, used deliberately. A single morning coffee, optionally paired with L-theanine for smoother focus, is reasonable for most adult students. Energy drinks with multi-stimulant blends and 300+ mg caffeine in a single serving are not.
- Omega-3 and a daily multivitamin during periods of poor eating (exam weeks, dorm food, irregular schedules). These maintain baseline status rather than producing acute improvements.
- Iron, B12, and vitamin D, if levels are low. For students with known deficiencies — common in young women with heavy periods, vegetarian/vegan students, and those with limited sun exposure — correction often produces the largest perceived improvement.
What students should not be doing in exam week
- Starting a new stimulant supplement they have never used before
- Taking prescription stimulants (Adderall, Ritalin, modafinil) without a prescription
- Mega-dosing caffeine with energy drinks
- Replacing sleep with supplements
A simple exam-week routine
Two to four weeks before the exam: confirm sleep regularity, daylight exposure, and adequate omega-3 and vitamin D status. During the week of the exam: maintain established habits, hydrate well, use a single morning caffeine with optional L-theanine, prioritize 7–9 hours of sleep, and stop studying 30–60 minutes before bed to allow cognitive wind-down.
The students who perform best are not the ones with the most supplements but the ones who slept seven to nine hours nightly across the study period.
Related Articles on HealthPerk
Explore more on this topic:
- Brain Fog Causes and Solutions
- How to Improve Focus Naturally
- How to Increase Concentration Fast
- Best Nootropics for Beginners
- L-Theanine vs Caffeine for Focus
- Foods for Brain Health
Frequently Asked Questions
What are the best supplements for focus and concentration adults can actually rely on?
For most adults, the reliable layer is: correct any documented deficiency (iron, B12, vitamin D, omega-3) first; add evidence-backed daily staples (omega-3 1–2 g/day, vitamin D as needed, creatine 3–5 g/day if tolerated); and use L-theanine plus moderate caffeine acutely before focused work. Almost everything beyond this list has smaller or contested evidence and should be trialed one variable at a time for 8–12 weeks before judging whether it helps.
Do supplements for brain fog that work for one person work for everyone?
No — supplements work best when matched to the underlying driver. Iron helps when ferritin is low, B12 helps when B12 is low, vitamin D helps when levels are deficient, and omega-3 helps especially in people with low baseline fish intake. Taking those same supplements when status is already adequate typically produces little to no perceptible effect. Identifying the driver through a basic blood panel is more useful than guessing which supplement to try.
What vitamins for memory and focus are most often deficient?
The most commonly deficient vitamins relevant to cognition are B12 (particularly in vegetarians, vegans, adults over 60, and people on metformin or acid suppressants), vitamin D (particularly in higher latitudes and people with limited sun exposure), and iron (particularly in menstruating women and frequent blood donors). These are inexpensive to test and inexpensive to correct, and correction often produces the most noticeable cognitive improvement of any supplement intervention.
Which supplements for cognitive function have the strongest 2026 evidence?
Omega-3 (EPA + DHA), creatine monohydrate, and the combination of L-theanine with caffeine have the strongest and most replicated evidence. Bacopa monnieri, rhodiola rosea, and lion's mane have moderate but more variable evidence. Most proprietary "nootropic blends" with undisclosed per-ingredient doses have weak evidence. The tier of a supplement should drive expectations: Tier 1 produces reliable modest effects, Tier 3 may help some individuals after long trials.
Are supplements for mental clarity better taken daily or only as needed?
The answer depends on the supplement. Daily-use supplements like omega-3, vitamin D, B-complex, and creatine operate by maintaining substrate or correcting slow deficiencies over weeks. Acute-use compounds like L-theanine + caffeine operate same-day for specific tasks. Mixing the two — taking creatine "as needed" or L-theanine daily but never around focus tasks — wastes both categories. Match the supplement to the timescale it actually works on.
What supplements for students focus are reasonable during exam season?
A reasonable exam-season supplement plan is conservative: maintain omega-3 and a daily multivitamin during periods of poor eating, ensure adequate hydration, use a single morning coffee optionally paired with L-theanine, and correct any pre-existing deficiencies in iron, B12, or vitamin D. Avoid starting new stimulant supplements in exam week, energy drinks with 300+ mg caffeine, and prescription stimulants without a diagnosis. Sleep duration and regularity outperform any supplement intervention.
Why don't more nootropics show up on the "best supplements for focus and concentration" lists?
Most nootropics marketed in 2026 fall into Tier 3 or Tier 4 evidence — moderate at best, often industry-funded, frequently sold as proprietary blends with undisclosed per-ingredient doses. The compounds with the strongest replicated evidence (omega-3, creatine, L-theanine + caffeine) are not exciting marketing material because they are inexpensive, widely available, and unbranded. The honest version of "best supplements" therefore looks unglamorous compared with the marketing layer that surrounds the category.
This article is for informational purposes only and does not constitute medical advice. Supplements can interact with medications and may be inappropriate during pregnancy, breastfeeding, or in the presence of certain medical conditions including kidney disease, liver disease, bleeding disorders, and thyroid disease. Consult a qualified healthcare provider before starting any supplement regimen, particularly if you are taking prescription medications. Always have suspected deficiencies confirmed by laboratory testing before beginning replacement-dose supplementation. Individual results may vary.
About the author The HealthPerk Editorial Team reviews nutritional and cognitive health research through evidence synthesis cross-referenced with peer-reviewed clinical trials, Cochrane reviews, and clinical practice guidelines. Our supplement content is reviewed for medical accuracy against current internal medicine and nutritional science standards. How we review →
References
Lomagno, K. A., Hu, F., Riddell, L. J., Booth, A. O., Szymlek-Gay, E. A., Nowson, C. A., & Byrne, L. K. (2014). Increasing iron and zinc in pre-menopausal women and its effects on mood and cognition: A systematic review. Nutrients, 6(11), 5117–5141. https://doi.org/10.3390/nu6115117
Supports: iron repletion improves cognitive symptoms in low-iron women, including in the absence of overt anemia
Smith, A. D., Refsum, H., Bottiglieri, T., Fenech, M., Hooshmand, B., McCaddon, A., ... & Obeid, R. (2018). Homocysteine and dementia: An international consensus statement. Journal of Alzheimer's Disease, 62(2), 561–570. https://doi.org/10.3233/JAD-171042
Supports: B12 and folate status influence cognitive function via homocysteine metabolism
Bhatti, A. B., Usman, M., & Ali, F. (2016). Vitamin supplementation as an adjuvant treatment for Alzheimer's disease. Journal of Clinical and Diagnostic Research, 10(8), OE07–OE11. https://doi.org/10.7860/JCDR/2016/20273.8348
Supports: rationale for vitamin status assessment in cognitive symptom workup
Avgerinos, K. I., Spyrou, N., Bougioukas, K. I., & Kapogiannis, D. (2018). Effects of creatine supplementation on cognitive function of healthy individuals: A systematic review of randomized controlled trials. Experimental Gerontology, 108, 166–173. https://doi.org/10.1016/j.exger.2018.04.013
Supports: creatine monohydrate produces measurable cognitive benefits in healthy adults, particularly under stress or sleep deprivation
Prokopidis, K., Giannos, P., Triantafyllidis, K. K., Kechagias, K. S., Forbes, S. C., & Candow, D. G. (2023). Effects of creatine supplementation on memory in healthy individuals: A systematic review and meta-analysis of randomized controlled trials. Nutrition Reviews, 81(4), 416–427. https://doi.org/10.1093/nutrit/nuac064
Supports: meta-analysis demonstrating improvements in short-term memory with creatine supplementation
Owen, G. N., Parnell, H., De Bruin, E. A., & Rycroft, J. A. (2008). The combined effects of L-theanine and caffeine on cognitive performance and mood. Nutritional Neuroscience, 11(4), 193–198. https://doi.org/10.1179/147683008X301513
Supports: L-theanine combined with caffeine improves attention and reduces caffeine-associated arousal
Bell, L., Lamport, D. J., Butler, L. T., & Williams, C. M. (2015). A review of the cognitive effects observed in humans following acute supplementation with flavonoids, and their associated mechanisms of action. Nutrients, 7(12), 10290–10306. https://doi.org/10.3390/nu7125538
Supports: dietary flavonoids and omega-3 fatty acids contribute to cognitive performance via vascular and inflammatory mechanisms
Bauer, I., Hughes, M., Rowsell, R., Cockerell, R., Pipingas, A., Crewther, S., & Crewther, D. (2014). Omega-3 supplementation improves cognition and modifies brain activation in young adults. Human Psychopharmacology: Clinical and Experimental, 29(2), 133–144. https://doi.org/10.1002/hup.2379
Supports: omega-3 supplementation improves cognitive performance and underlying brain activation in healthy young adults
Kongkeaw, C., Dilokthornsakul, P., Thanarangsarit, P., Limpeanchob, N., & Norman Scholfield, C. (2014). Meta-analysis of randomized controlled trials on cognitive effects of Bacopa monnieri extract. Journal of Ethnopharmacology, 151(1), 528–535. https://doi.org/10.1016/j.jep.2013.11.008
Supports: bacopa monnieri produces modest improvements in memory after 8–12 weeks of consistent supplementation
Ishaque, S., Shamseer, L., Bukutu, C., & Vohra, S. (2012). Rhodiola rosea for physical and mental fatigue: A systematic review. BMC Complementary and Alternative Medicine, 12, 70. https://doi.org/10.1186/1472-6882-12-70
Supports: rhodiola rosea has moderate evidence for reducing stress-related mental fatigue in adults
Frequently Asked Questions
What are the best supplements for focus and concentration adults can actually rely on?
Correct documented deficiencies first (iron, B12, vitamin D, omega-3), then add daily staples like omega-3 1-2 g/day, vitamin D as needed, and creatine 3-5 g/day if tolerated. Use L-theanine plus moderate caffeine acutely before focused work. Trial anything beyond this list one variable at a time for 8-12 weeks.
Do supplements for brain fog that work for one person work for everyone?
No. Supplements for brain fog work best when matched to the underlying driver. Iron helps when ferritin is low, B12 helps when B12 is low, vitamin D helps when deficient, and omega-3 helps especially in people with low fish intake. Taking those same supplements when status is already adequate produces little perceptible effect.
What vitamins for memory and focus are most often deficient?
The most commonly deficient vitamins relevant to cognition are B12 (in vegetarians, adults over 60, and people on metformin or acid suppressants), vitamin D (in higher latitudes and limited sun exposure), and iron (in menstruating women). These are inexpensive to test and correct.
Which supplements for cognitive function have the strongest 2026 evidence?
Omega-3 (EPA + DHA), creatine monohydrate, and the combination of L-theanine with caffeine have the strongest replicated evidence. Bacopa monnieri, rhodiola rosea, and lion's mane have moderate but more variable evidence. Most proprietary nootropic blends have weak evidence.
Are supplements for mental clarity better taken daily or only as needed?
Daily-use supplements like omega-3, vitamin D, B-complex, and creatine operate by maintaining substrate over weeks. Acute-use compounds like L-theanine + caffeine operate same-day for specific tasks. Match the supplement to the timescale it actually works on.
What supplements for students focus are reasonable during exam season?
Maintain omega-3 and a daily multivitamin, ensure hydration, use a single morning coffee optionally paired with L-theanine, and correct any pre-existing deficiencies in iron, B12, or vitamin D. Avoid starting new stimulant supplements in exam week and energy drinks with 300+ mg caffeine. Sleep outperforms any supplement intervention.
Why don't more nootropics show up on the best supplements for focus and concentration lists?
Most marketed nootropics fall into moderate or weak evidence tiers, often industry-funded and sold as proprietary blends with undisclosed doses. Compounds with the strongest evidence (omega-3, creatine, L-theanine + caffeine) are inexpensive and unbranded, which makes them less attractive as marketing material.
More from Supplements


