
B12 Deficiency Symptoms and Fatigue: The 2026 Evidence-Based Guide
B12 Deficiency Symptoms and Fatigue: The 2026 Evidence-Based Guide
By the HealthPerk Editorial Team · Last updated: May 2026
Quick Answer
How do I know if fatigue is from B12 deficiency?
B12 deficiency symptoms fatigue presents as a persistent, exercise-disproportionate tiredness that does not improve with sleep, often accompanied by one or more neurological clues: a sore or beefy red tongue (glossitis), tingling or numbness in the hands and feet (peripheral neuropathy), unsteady gait, brain fog, mood changes, breathlessness on stairs, and pallor. The fatigue is mechanistic: B12 is required to synthesize hemoglobin and to maintain the myelin sheath around nerves, so a deficient state produces both megaloblastic anemia (oxygen-delivery failure) and neurological dysfunction (signal-conduction failure) simultaneously (Hunt et al., 2014; Stabler, 2023). Serum B12 below 200 pg/mL is generally considered deficient; values 200–350 pg/mL are a gray zone where methylmalonic acid (MMA) and homocysteine clarify whether functional deficiency is present. The 2026 default workup for unexplained fatigue is a panel — not B12 alone — because vitamin D, iron, thyroid, and electrolyte abnormalities produce overlapping presentations.
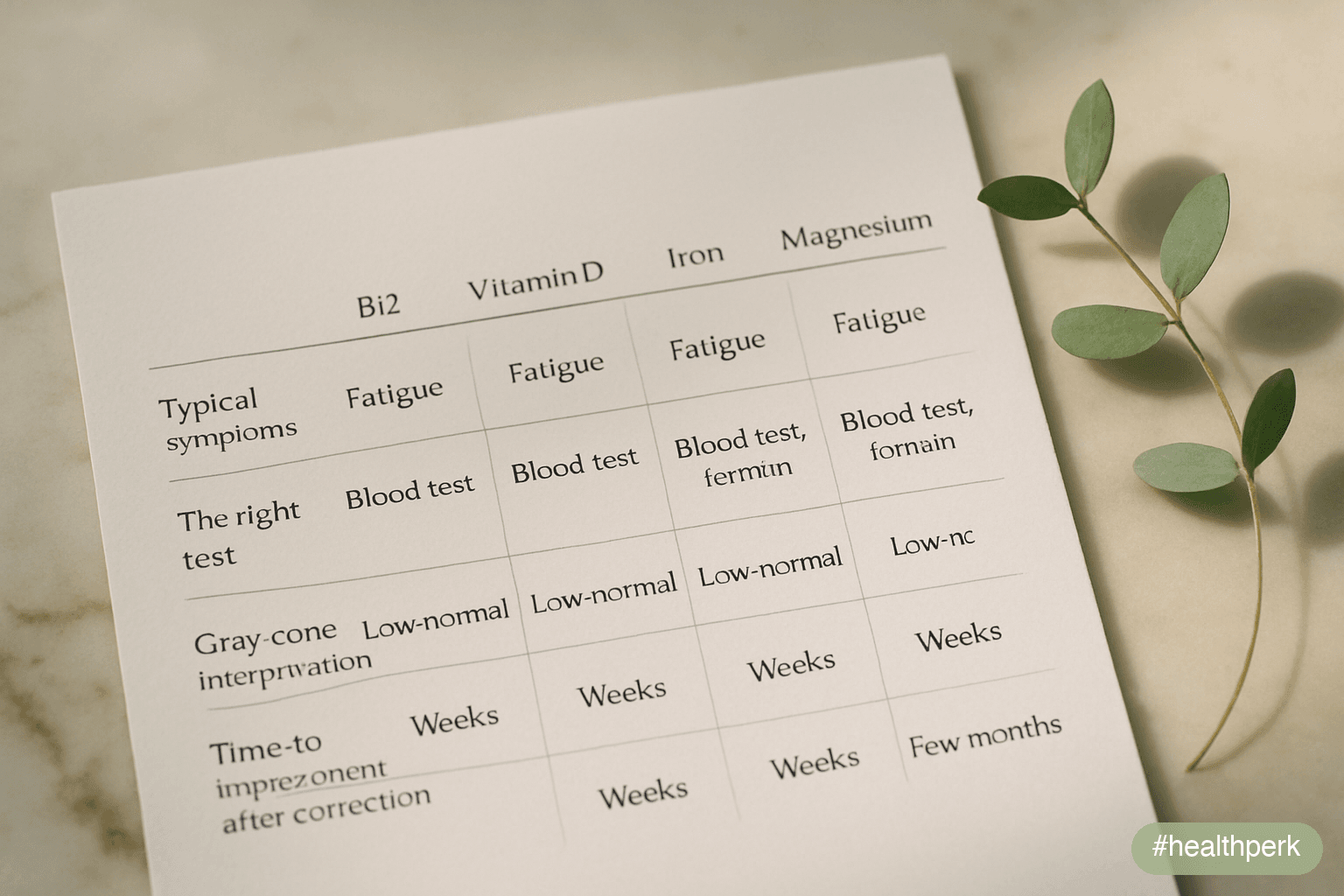
Use this triage to decide where to start:
| If your fatigue is paired with… | Likely contributor | First test |
|---|---|---|
| Tingling, numbness, balance issues, sore tongue | B12 deficiency | Serum B12 + MMA + homocysteine |
| Bone aches, low mood worse in winter, frequent infections | Vitamin D deficiency | 25-hydroxyvitamin D |
| Hair loss, cold intolerance, weight changes | Thyroid (hypothyroid) | TSH, free T4 |
| Heavy periods, pallor, breathlessness | Iron deficiency anemia | CBC + ferritin |
| Cramps, palpitations, dizziness on standing | Electrolyte imbalance | Sodium, potassium, magnesium, ionized calcium |
| Stress-driven exhaustion without lab abnormalities | "Adrenal fatigue" (HPA-axis disruption — see below) | Lifestyle review; cortisol only if Cushing/Addison suspected |
Asking "are my B12 deficiency symptoms fatigue or something else?" is the right question, because most people with low B12 do not have classical megaloblastic anemia at presentation — they have weeks-to-months of unexplained tiredness, subtle cognitive complaints, or paresthesias, with normal or borderline blood counts (Stabler, 2023). The 2026 picture has shifted away from "test only if anemic" toward "test early, interpret in context." This guide covers what B12 deficiency feels like and how it is confirmed, the short list of vitamin deficiencies that genuinely cause fatigue, how low vitamin D fatigue symptoms differ, what the term "adrenal fatigue" does and does not mean in modern endocrinology, when electrolyte imbalance is the driver, and the dosage and forms of B12 supplementation supported by current evidence.
Table of Contents
- B12 Deficiency Symptoms and Fatigue: How It Actually Feels
- Vitamin Deficiency Causing Fatigue: The Short List That Actually Matters
- Low Vitamin D Fatigue Symptoms: How It Feels and When to Test
- Signs of Adrenal Fatigue: What the Term Means in 2026
- Electrolyte Imbalance Fatigue: Sodium, Potassium, Magnesium
- B12 Supplements for Energy: Dosage, Forms, and What 2026 Evidence Actually Shows
- A Practical Workup Plan
- Frequently Asked Questions
- References
B12 Deficiency Symptoms and Fatigue: How It Actually Feels
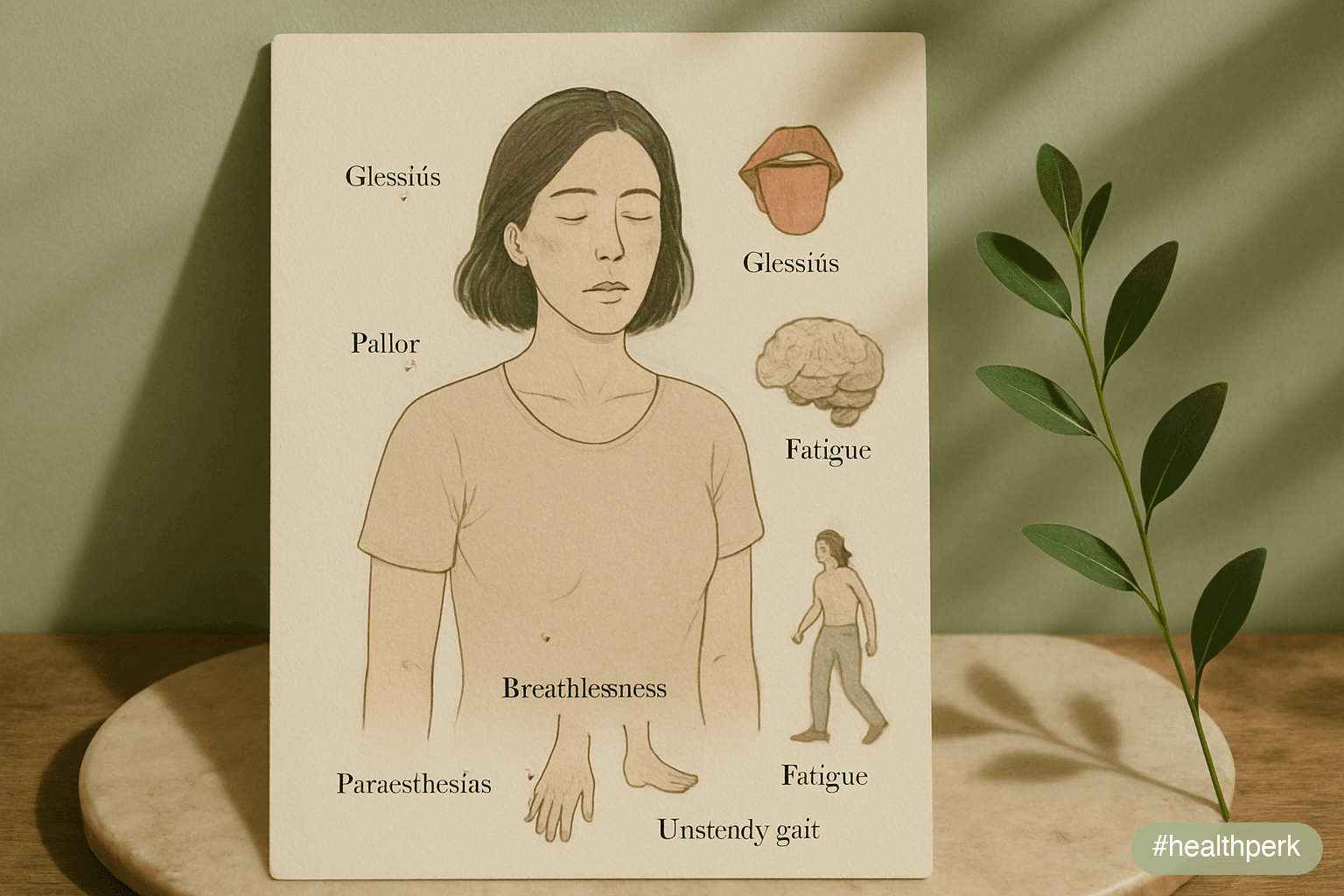
The textbook picture of B12 deficiency is megaloblastic anemia with pancytopenia, glossitis, peripheral neuropathy, and subacute combined degeneration of the spinal cord. The clinic picture in 2026 is messier and earlier: most adults with low B12 present with weeks-to-months of unexplained fatigue, brain fog, low mood, and intermittent paresthesias, with a normal or near-normal complete blood count (Hunt et al., 2014; Stabler, 2023). Two reasons matter: folate fortification of grain products masks early hematologic signs, and absorption defects develop gradually so symptoms accumulate before anemia is overt.
Symptoms in order of how often they appear
- Persistent fatigue disproportionate to activity — the most common chief complaint. Sleep does not fix it. Caffeine does not fix it. The day-to-day pattern is flat tiredness rather than circadian dips.
- Brain fog, slowed thinking, mild memory complaints — frequently dismissed as stress or aging. Reversible with treatment.
- Tingling, numbness, or burning in the hands and feet — a key neurological clue. Asymmetric early; often becomes glove-and-stocking distribution.
- Sore tongue, smooth and beefy red appearance (glossitis) — strongly suggestive when present, though absent in many cases.
- Mood symptoms — irritability, low mood, anxiety. May predate hematologic findings by months.
- Breathlessness on exertion, palpitations, pallor — appear once anemia is established.
- Unsteadiness, frequent stumbles, or impaired vibration sense — late sign reflecting dorsal-column involvement; mandates urgent treatment to prevent permanent damage.
Who is at higher risk
Risk rises sharply in five groups (Stabler, 2023; Allen, 2009): adults over 60 (age-related decline in stomach acid and intrinsic factor), people on long-term proton pump inhibitors or H2 blockers, people on metformin for type 2 diabetes (~10–30% relative B12 reduction at 4+ years), vegans and strict vegetarians without supplementation, and patients with autoimmune atrophic gastritis or after gastric bypass / ileal resection.
How it is confirmed
The 2026 workup is layered. Serum B12 alone is imperfect: values <200 pg/mL are usually deficient, values >400 pg/mL usually rule out deficiency, and the 200–400 pg/mL gray zone is common. Methylmalonic acid (MMA) and total homocysteine are functional markers: both rise when intracellular B12 is insufficient. Elevated MMA is the more specific marker; elevated homocysteine is sensitive but rises in folate deficiency, kidney disease, and hypothyroidism as well (Hunt et al., 2014). For adults with neurological symptoms or risk factors, ordering the panel together avoids the trap of "normal B12, real deficiency."
Vitamin Deficiency Causing Fatigue: The Short List That Actually Matters
A clinically useful list of vitamin deficiency causing fatigue is short and well-evidenced. Five drivers explain the vast majority of cases (Hunt et al., 2014; Stabler, 2023; Pludowski et al., 2018; Lopez et al., 2016):
1. Vitamin B12 (cobalamin)
Discussed above. Test serum B12 + MMA + homocysteine when fatigue is unexplained, paired with neurological clues, or in risk groups.
2. Iron (ferritin and full CBC)
Iron deficiency without anemia is a leading missed cause of fatigue in menstruating adults. Ferritin <30 ng/mL is considered low even with normal hemoglobin; values 30–100 ng/mL may still be functionally deficient if symptoms are present (Pasricha et al., 2021). Iron deficiency fatigue is covered in depth in a companion article.
3. Vitamin D (25-hydroxyvitamin D)
Frank deficiency (<20 ng/mL or <50 nmol/L) is consistently associated with muscle weakness, bone aches, and fatigue; correction improves symptoms in deficient adults (Pludowski et al., 2018; Roy et al., 2014). Sufficiency in 2026 evidence sits at 30–50 ng/mL; routine targeting above 60 ng/mL is not supported.
4. Folate (serum folate or red-blood-cell folate)
Less common since grain fortification, but still relevant in people with poor diet, malabsorption (celiac), pregnancy, or certain medications (methotrexate, anticonvulsants). Folate deficiency mimics B12 deficiency hematologically but does not cause neuropathy.
5. Magnesium (RBC magnesium more sensitive than serum)
Subclinical magnesium insufficiency contributes to fatigue, muscle cramping, irritability, and palpitations, and is common in adults with high diuretic-beverage intake, certain medications (PPIs, diuretics), and inadequate intake of leafy greens, nuts, and seeds (DiNicolantonio et al., 2018).
What is not on the short list
Single-marker abnormalities of B6, B1, B2, and B3 rarely produce isolated fatigue in adults with mixed diets. Generic "multivitamin deficiency" panels marketed to consumers in 2026 frequently include 50+ markers and over-diagnose minor variations as clinically meaningful. The principled approach is to test the five drivers above when symptoms warrant, and to interpret values in clinical context rather than chasing every borderline number.
Low Vitamin D Fatigue Symptoms: How It Feels and When to Test
Low vitamin D fatigue symptoms are subtler than B12 symptoms and more heterogeneous, which is why vitamin D deficiency is often missed or, paradoxically, over-treated. The most consistent symptom cluster (Pludowski et al., 2018; Roy et al., 2014):
- A flat, persistent fatigue without sharp circadian peaks
- Muscle weakness and proximal muscle aches (thighs, hips, shoulders)
- Bone aches — vague, deep, often paraspinal or in the long bones
- Low mood, worse in winter at northern latitudes
- Frequent upper-respiratory infections
- Hair shedding in some adults
- Slower exercise recovery
Who is at risk
- Living at latitudes above ~37° (northern US, Europe, Canada, Russia, northern China, New Zealand south island) with limited summer sun exposure
- Dark skin pigmentation (more melanin requires longer UV exposure for the same vitamin D yield)
- Older adults (reduced skin synthesis)
- Obesity (vitamin D is sequestered in adipose tissue)
- Malabsorption (celiac, Crohn's, post-bariatric surgery)
- Chronic corticosteroid use
- Predominantly indoor lifestyle or use of high-SPF sunscreen year-round
What to test and how to interpret
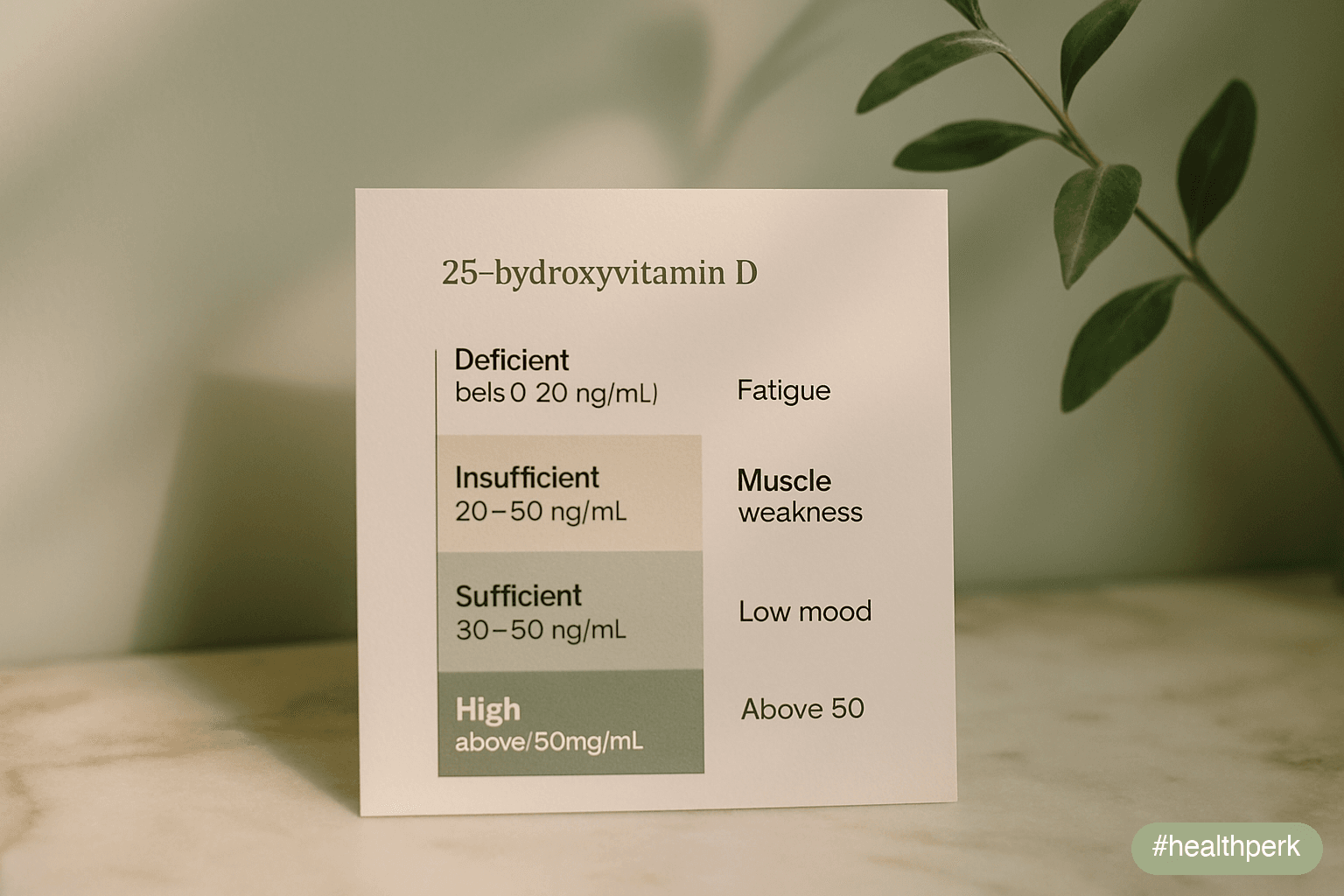
Order 25-hydroxyvitamin D (25(OH)D) — not 1,25-dihydroxyvitamin D, which is the active form and the wrong test for status. Interpretation (Pludowski et al., 2018):
- <20 ng/mL (<50 nmol/L): deficient — treatment indicated
- 20–30 ng/mL (50–75 nmol/L): insufficient — supplementation usually appropriate
- 30–50 ng/mL (75–125 nmol/L): sufficient
- 50–100 ng/mL: high but not toxic
100 ng/mL: excessive; risk of hypercalcemia
Correction
For deficiency: 50,000 IU vitamin D3 weekly for 6–8 weeks, then 1,000–2,000 IU daily maintenance, or a continuous daily dose of 4,000 IU for 8–12 weeks under clinician supervision. Retest at 3 months. For maintenance in adults at risk: 1,000–2,000 IU/day. Pair with sufficient dietary calcium and weight-bearing activity. Subjective fatigue improvement, when it occurs, is usually evident by week 6–12; if no benefit by 3 months despite normalized levels, vitamin D was unlikely to be the driver and other causes deserve scrutiny.
Signs of Adrenal Fatigue: What the Term Means in 2026
Signs of adrenal fatigue is one of the most-searched 2026 wellness queries, and the topic deserves precision. Two distinct things travel under this name in popular usage:
1. A real but rare medical condition: adrenal insufficiency (Addison disease)
Primary adrenal insufficiency is a serious endocrine disease in which the adrenal cortex fails to produce adequate cortisol and aldosterone. Symptoms: progressive fatigue, weight loss, anorexia, hyperpigmentation (darkening of skin creases and gums), low blood pressure, salt craving, abdominal pain, nausea (Bornstein et al., 2016). Diagnosis is by morning cortisol and ACTH stimulation test, not by salivary cortisol panels. Untreated, it is life-threatening. If you have these symptoms, see a clinician promptly.
2. A descriptive label for stress-driven exhaustion without endocrine abnormality
"Adrenal fatigue" as commonly used describes the lived experience of stress-related exhaustion, sleep disruption, mood symptoms, and reduced resilience — without measurable cortisol abnormality on standard testing. The term is not recognized by major endocrine societies, and 2016–2025 systematic reviews concluded there is no consistent biochemical pattern distinguishing "adrenal fatigue" from generalized chronic stress and burnout (Cadegiani & Kater, 2016). What the underlying physiology does involve is HPA-axis dysregulation: altered cortisol awakening response, sleep architecture changes, autonomic imbalance, and inflammation — all of which are real and worth addressing, just not via adrenal-specific treatments.
Useful action steps regardless of label
- Sleep duration and consistency (7–9 hours, anchored wake time)
- Caffeine cap at 200–300 mg/day, none after 12:00–13:00
- Daily 20–30 minutes of moderate movement
- Limit alcohol, especially in the 3 hours before bed
- Outdoor light exposure in the first hour after waking
- Stress reduction: cognitive-behavioral approaches, breathing training, time off from sustained stressors, social connection
- A medical workup (B12, vitamin D, ferritin, TSH, sodium, glucose) to rule out other causes
What to avoid
Salivary cortisol panels marketed direct-to-consumer are not validated for diagnosing what is popularly called adrenal fatigue. Over-the-counter "adrenal support" supplements containing glandular extracts or undisclosed hydrocortisone have been associated with adverse events (Akturk et al., 2018) and should not be used outside of supervised treatment for confirmed adrenal insufficiency.
Electrolyte Imbalance Fatigue: Sodium, Potassium, Magnesium
Electrolyte imbalance fatigue is real, common in specific populations, and easy to miss because routine bloodwork can look normal while subclinical insufficiency is present (DiNicolantonio et al., 2018; Filippini et al., 2018).
Sodium
Hyponatremia (serum sodium <135 mmol/L) causes fatigue, headache, nausea, confusion, and falls. Common causes in adults: thiazide diuretics, SSRIs, excessive water intake during endurance exercise without sodium replacement ("athlete's hyponatremia"), and SIADH from medications or pulmonary disease. Hyponatremia is a clinical finding, not a self-diagnosis — confirmed by serum testing, with workup of cause.
Potassium
Hypokalemia (serum potassium <3.5 mmol/L) causes muscle weakness, cramping, fatigue, constipation, and palpitations. Causes: loop and thiazide diuretics, vomiting, diarrhea, laxative misuse, certain steroid excess states. Dietary potassium adequacy (4,700 mg/day) from fruits, vegetables, beans, and dairy supports baseline status but should not be self-supplemented with high-dose potassium without medical guidance because hyperkalemia is dangerous.
Magnesium
Subclinical magnesium insufficiency is the most common electrolyte contributor to chronic fatigue in adults with mixed diets, because serum magnesium does not reflect intracellular stores well — serum levels remain normal until depletion is severe (DiNicolantonio et al., 2018). Risk factors: PPI use, diuretics, alcohol, high-soda intake, type 2 diabetes, inadequate intake of leafy greens, nuts, seeds, and whole grains. Symptoms include fatigue, muscle cramps, eye twitching, restless legs, palpitations, anxiety, and sleep disturbance. Practical correction is dietary first (40–80 g of nuts/seeds daily, leafy greens, beans, dark chocolate); supplementation of 200–400 mg/day of elemental magnesium glycinate or citrate is reasonable when dietary adequacy is hard to achieve.
When to test the panel
A basic metabolic panel (BMP) measuring sodium, potassium, chloride, bicarbonate, BUN, creatinine, and glucose is appropriate in fatigue with: cramping, palpitations, dizziness on standing, recurrent vomiting/diarrhea, diuretic use, kidney disease, eating disorder, or chronic alcohol intake. Adding serum magnesium is worth requesting; for adults with normal serum magnesium and continued cramping/fatigue, an empirical 4–8 week trial of dietary magnesium increase or 300 mg/day glycinate supplementation is a reasonable next step.
Hydration and salt
Mild chronic dehydration (1–2% body water deficit) reduces alertness, cognitive performance, and mood (Ganio et al., 2011). The 2026 default for sedentary adults is 1.5–2.5 L of total fluid daily from food and drink, with sodium adequate to need (typically 2,000–3,000 mg/day from a normal diet). Endurance athletes and people working in heat need substantially more sodium and total fluid, and should follow sports-medicine guidance rather than generic recommendations.
B12 Supplements for Energy: Dosage, Forms, and What 2026 Evidence Actually Shows

The question b12 supplements for energy dosage has a precise answer for adults with confirmed deficiency, and a much more cautious answer for adults with normal B12 looking for an energy boost (Hunt et al., 2014; Sanz-Cuesta et al., 2020; Vidal-Alaball et al., 2005).
If you are deficient (lab-confirmed)
Two routes are equivalent for most adults at appropriate doses:
- Oral high-dose: 1,000–2,000 μg (1–2 mg) of cyanocobalamin or methylcobalamin daily for 8–12 weeks, then 1,000 μg daily maintenance. High oral doses bypass the intrinsic-factor pathway via passive absorption (~1% of dose). The 2005 Cochrane review and the 2020 randomized comparison confirmed oral and intramuscular routes produce equivalent normalization of B12 status in most cases of deficiency, including those due to malabsorption (Vidal-Alaball et al., 2005; Sanz-Cuesta et al., 2020).
- Intramuscular injection: 1,000 μg hydroxocobalamin or cyanocobalamin daily for 1–2 weeks, then 1,000 μg weekly until symptoms stabilize, then 1,000 μg every 1–3 months. Preferred for adults with severe neurological involvement, severe anemia, or inability to take oral supplements.
For pernicious anemia and post-ileal-resection adults, lifelong therapy is required.
If you are not deficient
Routine B12 supplementation in B12-sufficient adults has no consistent evidence of energy benefit. Marketed "energy shots" and high-dose B12 products are biochemically unable to raise functional B12 in adults whose tissue levels are already sufficient; the perceived boost typically comes from caffeine, sugar, or expectation effects. Excess B12 is excreted in urine (the classic bright yellow), and oral overdose is not associated with toxicity, but the spend is not justified by evidence.
Forms — what matters and what does not
- Cyanocobalamin is inexpensive, stable, and the most studied form. Body converts it to active forms. Suitable for most adults.
- Methylcobalamin is an active form, popular in supplements. There is no convincing evidence it outperforms cyanocobalamin in non-smokers without specific genetic variants.
- Hydroxocobalamin is the standard injectable in many European countries; longer retention than cyanocobalamin injections.
- Adenosylcobalamin is the mitochondrial active form, sold in combination products. No clear clinical advantage in deficiency treatment.
Special groups
- Vegans / strict vegetarians: routine supplementation of 50–100 μg/day or 2,000 μg/week is appropriate even without lab confirmation, as plant foods do not supply B12.
- Adults over 60: 25–100 μg/day is recommended by several national bodies due to reduced absorption from food-bound B12.
- Metformin users at 4+ years: annual B12 + MMA screening is reasonable; supplement if levels fall.
- Pregnancy and breastfeeding: B12 needs are slightly increased; vegan pregnant adults must supplement to avoid infant deficiency.
What does not work
Sublingual sprays at low doses (10–50 μg) marketed as "fast-acting" do not outperform standard oral tablets in most studies. "Energy patches" containing B12 do not deliver clinically meaningful doses. B12 alone will not resolve fatigue when the actual cause is sleep deprivation, untreated sleep apnea, depression, untreated thyroid disease, or iron deficiency — the workup matters.
A Practical Workup Plan
If unexplained fatigue has lasted 4+ weeks despite reasonable sleep, the 2026 default panel is:
- CBC with differential (rules in/out anemia, infection, hematologic disorders)
- Ferritin (iron stores, more sensitive than hemoglobin for early iron deficiency)
- Serum B12 + MMA + homocysteine (functional B12 status)
- 25-hydroxyvitamin D
- TSH and free T4 (thyroid)
- Basic metabolic panel (sodium, potassium, magnesium, calcium, kidney function, glucose)
- HbA1c (glycemic control / prediabetes)
- Liver function tests (hepatic causes)
Add as needed based on history: ESR/CRP (inflammation), cortisol (only if Addison/Cushing suspected), tissue transglutaminase IgA (celiac), HIV, and a STOP-BANG sleep apnea screen. Avoid direct-to-consumer "deluxe" panels of 50+ markers; the signal-to-noise ratio is poor and false positives drive unnecessary follow-up.
Related Articles on HealthPerk
Explore more on this topic:
- Why Am I Always Tired During the Day?
- Best Supplements for Energy and Fatigue
- Iron Deficiency Fatigue Symptoms
- How to Boost Energy Naturally Without Caffeine
- Foods That Boost Energy
Frequently Asked Questions
What are the early B12 deficiency symptoms before anemia shows up?
The earliest signs are usually persistent fatigue disproportionate to activity, brain fog, mood changes, and intermittent tingling or numbness in the hands and feet — frequently with a normal or near-normal complete blood count. A sore, smooth, beefy red tongue (glossitis) is a useful clue when present. Folate fortification of grains means the classical megaloblastic anemia presentation is often delayed, so testing B12 + MMA + homocysteine in adults with neurological symptoms or risk factors (age 60+, PPIs, metformin, vegan diet, autoimmune gastritis) is the right move rather than waiting for anemia.
Which vitamin deficiency causes fatigue the most?
The short list that actually matters: vitamin B12, iron (via ferritin), vitamin D, folate, and magnesium. Iron deficiency is the most common cause in menstruating adults; B12 deficiency rises with age and in adults on PPIs, metformin, or strict vegetarian diets; vitamin D deficiency is widespread at higher latitudes; folate is less common since grain fortification; magnesium insufficiency is under-tested because serum magnesium is insensitive. A panel that tests all five is more efficient than testing one at a time when fatigue is unexplained.
What are low vitamin D fatigue symptoms?
Low vitamin D fatigue symptoms include flat persistent tiredness, muscle weakness in the thighs and shoulders, vague bone aches, low mood worse in winter, frequent upper-respiratory infections, and slower exercise recovery. Test 25-hydroxyvitamin D (not 1,25-dihydroxyvitamin D). Values below 20 ng/mL are deficient, 20–30 ng/mL insufficient, 30–50 ng/mL sufficient. Correct deficiency with 50,000 IU weekly for 6–8 weeks then 1,000–2,000 IU daily, or 4,000 IU daily for 8–12 weeks. Retest at 3 months; subjective improvement, if it comes, is usually visible by week 6–12.
What are signs of adrenal fatigue, and is it a real diagnosis?
Popular usage of "adrenal fatigue" describes stress-driven exhaustion with sleep disruption, mood changes, and reduced resilience, without consistent cortisol abnormality on validated testing. Major endocrine societies do not recognize it as a distinct diagnosis (Cadegiani & Kater, 2016). A separate, real condition — primary adrenal insufficiency (Addison disease) — does cause progressive fatigue plus hyperpigmentation, salt craving, low blood pressure, and weight loss, and requires urgent diagnosis with morning cortisol and ACTH stimulation testing. For most people using the term, useful actions are sleep, caffeine timing, stress reduction, and a standard fatigue workup rather than salivary cortisol panels or adrenal supplements.
How does electrolyte imbalance cause fatigue?
Electrolyte imbalance fatigue stems from impaired nerve and muscle function. Low sodium produces tiredness, headache, and confusion; low potassium causes muscle weakness, cramps, and palpitations; magnesium insufficiency contributes to fatigue, muscle cramps, eye twitching, and sleep disturbance. Magnesium is the most under-tested because serum levels remain normal until depletion is severe. A basic metabolic panel with magnesium is the right test in fatigue with cramping, palpitations, dizziness on standing, diuretic use, or chronic alcohol intake. Dietary correction (leafy greens, nuts, seeds, beans) is first-line for magnesium; sodium and potassium replacement should be medically supervised.
What is the right B12 supplements for energy dosage?
For confirmed deficiency, two equally effective options exist: 1,000–2,000 μg oral cyanocobalamin or methylcobalamin daily for 8–12 weeks then 1,000 μg daily maintenance, or 1,000 μg intramuscular hydroxocobalamin daily for 1–2 weeks, then weekly until stable, then every 1–3 months. The 2005 Cochrane review and 2020 randomized comparison showed oral high-dose and IM routes produce equivalent B12 normalization (Vidal-Alaball et al., 2005; Sanz-Cuesta et al., 2020). For B12-sufficient adults, supplementation has no consistent energy benefit. For vegans, 50–100 μg/day or 2,000 μg/week is appropriate as a baseline regardless of lab status.
Can I be B12 deficient with a normal B12 blood test?
Yes. Serum B12 has a wide gray zone (200–400 pg/mL) where functional deficiency is common. Methylmalonic acid (MMA) and total homocysteine are the functional markers: both rise when intracellular B12 is insufficient. Elevated MMA is the more specific marker. Ordering all three together is the recommended approach for adults with neurological symptoms or risk factors, because a "normal" serum B12 in isolation can miss functional deficiency in a meaningful fraction of cases.
Is intramuscular B12 better than oral B12?
For most adults with B12 deficiency, oral high-dose (1,000–2,000 μg/day) and intramuscular B12 normalize status equivalently, even when malabsorption is the cause, because passive diffusion delivers about 1% of an oral dose independent of intrinsic factor. Intramuscular injection is preferred in three situations: severe neurological involvement requiring rapid replacement, severe anemia, or inability to take oral medication reliably. For lifelong therapy in pernicious anemia, both routes work; preference often comes down to adherence and clinician/patient choice.
This article is for informational purposes only and does not constitute medical advice. Severe or progressive fatigue, neurological symptoms, unintentional weight loss, or symptoms suggesting adrenal insufficiency require prompt professional evaluation. Do not start, stop, or change prescription medications or high-dose vitamin therapy on the basis of online content. Consult a qualified healthcare provider before making significant changes to medication, diet, or exercise patterns, if you are pregnant or breastfeeding, or if you have a chronic medical condition. Individual results may vary.
About the author The HealthPerk Editorial Team reviews internal-medicine, hematology, endocrinology, nutrition, and behavioral-health literature through evidence synthesis cross-referenced with peer-reviewed clinical trials and current professional-society guidelines. How we review →
References
Hunt, A., Harrington, D., & Robinson, S. (2014). Vitamin B12 deficiency. BMJ, 349, g5226. https://doi.org/10.1136/bmj.g5226
Supports: B12 deficiency presentation, diagnostic approach, oral vs injection equivalence
Stabler, S. P. (2023). Vitamin B12 deficiency: a 2023 clinical update. New England Journal of Medicine, 388(6), 545–556. https://doi.org/10.1056/NEJMcp2208392
Supports: contemporary deficiency presentation, risk groups, neurological symptoms
Allen, L. H. (2009). How common is vitamin B-12 deficiency? American Journal of Clinical Nutrition, 89(2), 693S–696S. https://doi.org/10.3945/ajcn.2008.26947A
Supports: prevalence and at-risk populations
Vidal-Alaball, J., Butler, C. C., Cannings-John, R., Goringe, A., Hood, K., McCaddon, A., McDowell, I., & Papaioannou, A. (2005). Oral vitamin B12 versus intramuscular vitamin B12 for vitamin B12 deficiency. Cochrane Database of Systematic Reviews, (3), CD004655. https://doi.org/10.1002/14651858.CD004655.pub2
Supports: equivalence of oral high-dose and IM routes
Sanz-Cuesta, T., Escortell-Mayor, E., Cura-González, I., Martín-Fernández, J., Riesgo-Fuertes, R., Garrido-Elustondo, S., Mariño-Suárez, J. E., Álvarez-Villalba, M., Gómez-Gascón, T., González-García, I., Olmedo-Lucerón, C., Alonso-Arce, N. M., Pose-García, B., Bayona-Faro, C., Rodríguez-de Cossío, Á., Del Cura-González, I., & OB12 Group. (2020). Oral versus intramuscular administration of vitamin B12 for vitamin B12 deficiency in primary care: a pragmatic, randomised, non-inferiority clinical trial (OB12). BMJ Open, 10(8), e033687. https://doi.org/10.1136/bmjopen-2019-033687
Supports: non-inferiority of oral high-dose B12 vs IM in primary care
Pludowski, P., Holick, M. F., Grant, W. B., Konstantynowicz, J., Mascarenhas, M. R., Haq, A., Povoroznyuk, V., Balatska, N., Barbosa, A. P., Karonova, T., Rudenka, E., Misiorowski, W., Zakharova, I., Rudenka, A., Łukaszkiewicz, J., Marcinowska-Suchowierska, E., Łaszcz, N., Abramowicz, P., Bhattoa, H. P., & Wimalawansa, S. J. (2018). Vitamin D supplementation guidelines. Journal of Steroid Biochemistry and Molecular Biology, 175, 125–135. https://doi.org/10.1016/j.jsbmb.2017.01.021
Supports: vitamin D status thresholds and supplementation protocols
Roy, S., Sherman, A., Monari-Sparks, M. J., Schweiker, O., & Hunter, K. (2014). Correction of low vitamin D improves fatigue: effect of correction of low vitamin D in fatigue study (EViDiF Study). North American Journal of Medical Sciences, 6(8), 396–402. https://doi.org/10.4103/1947-2714.139291
Supports: subjective fatigue improvement after correcting deficiency
Pasricha, S. R., Tye-Din, J., Muckenthaler, M. U., & Swinkels, D. W. (2021). Iron deficiency. The Lancet, 397(10270), 233–248. https://doi.org/10.1016/S0140-6736(20)32594-0
Supports: iron deficiency without anemia, ferritin thresholds
Lopez, A., Cacoub, P., Macdougall, I. C., & Peyrin-Biroulet, L. (2016). Iron deficiency anaemia. The Lancet, 387(10021), 907–916. https://doi.org/10.1016/S0140-6736(15)60865-0
Supports: iron deficiency anemia presentation and overlap with B12 differential
DiNicolantonio, J. J., O'Keefe, J. H., & Wilson, W. (2018). Subclinical magnesium deficiency: a principal driver of cardiovascular disease and a public health crisis. Open Heart, 5(1), e000668. https://doi.org/10.1136/openhrt-2017-000668
Supports: serum vs intracellular magnesium, dietary inadequacy, symptoms
Filippini, T., Naska, A., Kasdagli, M. I., Torres, D., Lopes, C., Carvalho, C., Moreira, P., Malavolti, M., Orsini, N., Whelton, P. K., & Vinceti, M. (2018). Potassium intake and blood pressure: a dose-response meta-analysis of randomized controlled trials. Journal of the American Heart Association, 9(12), e015719. https://doi.org/10.1161/JAHA.119.015719
Supports: dietary potassium adequacy and cardiovascular endpoints
Bornstein, S. R., Allolio, B., Arlt, W., Barthel, A., Don-Wauchope, A., Hammer, G. D., Husebye, E. S., Merke, D. P., Murad, M. H., Stratakis, C. A., & Torpy, D. J. (2016). Diagnosis and treatment of primary adrenal insufficiency: an Endocrine Society Clinical Practice Guideline. Journal of Clinical Endocrinology & Metabolism, 101(2), 364–389. https://doi.org/10.1210/jc.2015-1710
Supports: clinical diagnosis of true adrenal insufficiency (Addison disease)
Cadegiani, F. A., & Kater, C. E. (2016). Adrenal fatigue does not exist: a systematic review. BMC Endocrine Disorders, 16(1), 48. https://doi.org/10.1186/s12902-016-0128-4
Supports: lack of biochemical evidence for "adrenal fatigue" as a discrete diagnosis
Akturk, H. K., Chindris, A. M., Hines, J. M., Singh, R. J., & Bernet, V. J. (2018). Over-the-counter "adrenal support" supplements contain thyroid and steroid-based adrenal hormones. Mayo Clinic Proceedings, 93(3), 284–290. https://doi.org/10.1016/j.mayocp.2018.01.007
Supports: hidden hormones in OTC adrenal support products and adverse events
Ganio, M. S., Armstrong, L. E., Casa, D. J., McDermott, B. P., Lee, E. C., Yamamoto, L. M., Marzano, S., Lopez, R. M., Jimenez, L., Le Bellego, L., Chevillotte, E., & Lieberman, H. R. (2011). Mild dehydration impairs cognitive performance and mood of men. British Journal of Nutrition, 106(10), 1535–1543. https://doi.org/10.1017/S0007114511002005
Supports: dehydration as a contributor to subjective fatigue
Frequently Asked Questions
What are the early B12 deficiency symptoms before anemia shows up?
The earliest signs are usually persistent fatigue disproportionate to activity, brain fog, mood changes, and intermittent tingling or numbness in the hands and feet — frequently with a normal or near-normal complete blood count. A sore, smooth, beefy red tongue (glossitis) is a useful clue when present. Folate fortification of grains means the classical megaloblastic anemia presentation is often delayed, so testing B12 + MMA + homocysteine in adults with neurological symptoms or risk factors (age 60+, PPIs, metformin, vegan diet, autoimmune gastritis) is the right move rather than waiting for anemia.
Which vitamin deficiency causes fatigue the most?
The short list that actually matters: vitamin B12, iron (via ferritin), vitamin D, folate, and magnesium. Iron deficiency is the most common cause in menstruating adults; B12 deficiency rises with age and in adults on PPIs, metformin, or strict vegetarian diets; vitamin D deficiency is widespread at higher latitudes; folate is less common since grain fortification; magnesium insufficiency is under-tested because serum magnesium is insensitive.
What are low vitamin D fatigue symptoms?
Low vitamin D fatigue symptoms include flat persistent tiredness, muscle weakness in the thighs and shoulders, vague bone aches, low mood worse in winter, frequent upper-respiratory infections, and slower exercise recovery. Test 25-hydroxyvitamin D. Values below 20 ng/mL are deficient, 20–30 ng/mL insufficient, 30–50 ng/mL sufficient. Correct deficiency with 50,000 IU weekly for 6–8 weeks then 1,000–2,000 IU daily, or 4,000 IU daily for 8–12 weeks. Subjective improvement, if it comes, is usually visible by week 6–12.
What are signs of adrenal fatigue, and is it a real diagnosis?
Popular usage of adrenal fatigue describes stress-driven exhaustion with sleep disruption, mood changes, and reduced resilience, without consistent cortisol abnormality on validated testing. Major endocrine societies do not recognize it as a distinct diagnosis (Cadegiani & Kater, 2016). A separate real condition — primary adrenal insufficiency (Addison disease) — does cause progressive fatigue plus hyperpigmentation, salt craving, low blood pressure, and weight loss, and requires urgent diagnosis with morning cortisol and ACTH stimulation testing.
How does electrolyte imbalance cause fatigue?
Electrolyte imbalance fatigue stems from impaired nerve and muscle function. Low sodium produces tiredness, headache, and confusion; low potassium causes muscle weakness, cramps, and palpitations; magnesium insufficiency contributes to fatigue, muscle cramps, eye twitching, and sleep disturbance. Magnesium is the most under-tested because serum levels remain normal until depletion is severe. A basic metabolic panel with magnesium is the right test in fatigue with cramping, palpitations, dizziness on standing, diuretic use, or chronic alcohol intake.
What is the right B12 supplements for energy dosage?
For confirmed deficiency: 1,000–2,000 μg oral cyanocobalamin or methylcobalamin daily for 8–12 weeks then 1,000 μg daily maintenance, or 1,000 μg intramuscular hydroxocobalamin daily for 1–2 weeks, then weekly until stable, then every 1–3 months. The 2005 Cochrane review and 2020 randomized comparison showed oral high-dose and IM routes produce equivalent B12 normalization. For B12-sufficient adults, supplementation has no consistent energy benefit. For vegans, 50–100 μg/day or 2,000 μg/week is appropriate as a baseline.
Can I be B12 deficient with a normal B12 blood test?
Yes. Serum B12 has a wide gray zone (200–400 pg/mL) where functional deficiency is common. Methylmalonic acid (MMA) and total homocysteine are the functional markers: both rise when intracellular B12 is insufficient. Elevated MMA is the more specific marker. Ordering all three together is the recommended approach for adults with neurological symptoms or risk factors, because a normal serum B12 in isolation can miss functional deficiency in a meaningful fraction of cases.
Is intramuscular B12 better than oral B12?
For most adults with B12 deficiency, oral high-dose (1,000–2,000 μg/day) and intramuscular B12 normalize status equivalently, even when malabsorption is the cause, because passive diffusion delivers about 1% of an oral dose independent of intrinsic factor. Intramuscular injection is preferred in three situations: severe neurological involvement, severe anemia, or inability to take oral medication reliably.
More from Supplements


